
Migration and Health: A Framework for 21st Century Policy-Making
article has not abstract
Published in the journal:
. PLoS Med 8(5): e32767. doi:10.1371/journal.pmed.1001034
Category:
Policy Forum
doi:
https://doi.org/10.1371/journal.pmed.1001034
Summary
article has not abstract
Summary Points
-
Migration is a global phenomenon that influences the health of individuals and populations.
-
Policy-making on migration and health is conducted within sector silos that frequently have different goals. Population mobility is wholly compatible with health-promoting strategies for migrants if decision-makers coordinate across borders and policy sectors.
-
Policies to protect migrant and public health will be most effective if they address the multiple phases of the migratory process, including pre-departure, travel, destination, interception, and return. Health intervention opportunities exist at each stage.
-
This article forms the introduction to a PLoS Medicine series on Migration & Health, laying out a new framework for understanding the migratory process and the five phases of migration, which are discussed in depth in five subsequent articles.
This is one article in a six-part PLoS Medicine series on Migration & Health.
Introduction
With an estimated 214 million people on the move internationally and approximately three-quarters of a billion people migrating within their own country, there can be little doubt that population mobility is among the leading policy issues of the 21st century [1]–[3]. Human migration is not a new phenomenon, but it has changed significantly in number and nature with the growth of globalization, including the ease of international transport and communication, the push and pull factors of shifting capital, effects of climate change, and periodic political upheaval, including armed conflict. As a result, migrant networks that facilitate mobility and circular migration, in particular, have expanded in unprecedented ways [4],[5]. Yet, there has not been commensurate development of coordinated policy approaches to address the health implications associated with modern migration. Internationally, policy-making on migration has generally been conducted from policy sector “silos” (e.g., international aid, security, immigration enforcement, trade, and labor) that rarely include the health sector and which often have different, if not incompatible, goals [6],[7]. As discussions on “global migration governance” and “global health governance” expand, it will be increasingly important for policy-makers to engage in cross-sector coordination and move beyond narrow protectionist policy approaches, such as migrant-screening, and the simplistic view of migration as a one-way trajectory [8].
Health policy-making in the context of migration has generally been viewed either in terms of its “threats” to public health or from a rights-based approach that focuses on health hazards faced by individual migrants and the associated service challenges [9]. The former lens dates back to medieval quarantine measures and prioritizes public health security and communicable disease control, relying heavily on monitoring and screening (e.g., tuberculosis, pandemic flu). The rights-based perspective is more recent and grounded in medical ethics. It recognizes migrants' special vulnerability to, for example, interpersonal and occupational hazards, social exclusion, and discrimination, and the importance of universal access and culturally competent health care services [10].
Although often framed as a “threat”, human mobility is not inherently risk-laden. However, poor policy coordination and contradictory policy goals, such as increasing foreign labor requirements while maintaining restrictive rights for migrants, can exacerbate risk conditions related to migration and pose health challenges [11],[12].
This paper presents an introduction to the PLoS Medicine series on migration and health (http://www.ploscollections.org/migrationhealth). It lays out a migratory process framework (Figure 1) that highlights the multistaged and cumulative nature of the health risks and intervention opportunities that can occur throughout the migration process, and points to the potential benefits of policy-making that spans the full range of migratory movement. Five subsequent articles in the series discuss in-depth the health impacts and policy needs associated with the five phases of this migratory process: pre-departure, travel, destination, interception, and return.

Global Estimates, Migrant Categories, and Gender
Theories and definitions of migration are diverse and include temporary and more permanent forms of human mobility that can occur for different purposes over long and short distances [13],[14]. Statistics on global migration are imprecise because of the diversity in definitions and due to the difficulty of counting irregular or undocumented migrants [15]. Table 1 presents some commonly used definitions and recent estimates for different mobile populations. Notably, internal migrants account for nearly four times as many individuals as international migrants. Among international migrants, it is estimated that nearly 50% of international movement is inter-regional [1].
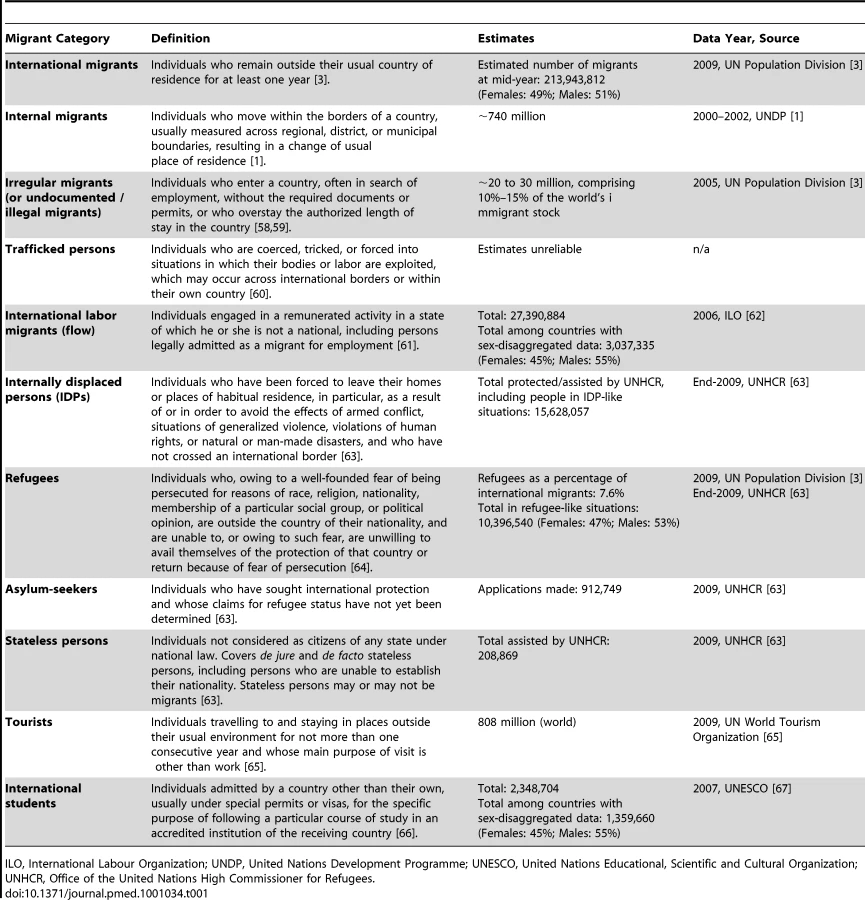
For the past 50 years, there have been an approximately equal proportion of migrant women and men [2]. The motives and conditions of women's migration have changed markedly, with a growing number of women migrating independently for low-skill labor opportunities, rather than as spousal or family dependents. This has raised discussions about the “feminization of migration” [16]. At the same time as numerous women may gain greater independence and empowerment through migration, particular risks may arise such as, physical and sexual violence, including trafficking for forced sex work [17].
In migration statistics, it is not uncommon for different mobile groups and males and females to be classified together as “immigrants” or categorized solely by nationality [18],[19]. But people frequently fit into multiple categories or change their migration status over time and circumstances. From a public health policy perspective, an important dichotomy is between “documented” versus “irregular” and “forced” migrants. Individuals who travel via legal channels with required documentation, e.g., high-skilled laborers, are likely to encounter fewer health risks and have better service access than undocumented or “irregular” migrants [20].
Phases of the Migratory Process and Health Considerations
Traditionally, policy-making has viewed migration as individual movement from point A to point B, generally focusing on permanent transnational resettlement. Yet, contemporary mobility is a much more complex process, more accurately viewed as a multistage cycle that can be entered into multiple times, in various ways, and may occur within or across national borders. Figure 1 depicts a migratory process model with five phases: pre-departure, travel, destination, interception (affecting a minority of migrants), and return [13],[21],[22]. This framework lends itself to more comprehensive and multinational policy-making. The five subsequent articles in the PLoS Medicine series will discuss in-depth these five phases, but here we provide a summary.
Pre-Departure Phase
The pre-departure phase comprises the time before individuals leave from their place of origin. Factors that may influence health at this stage include biological characteristics, local chronic disease patterns and pathogens, environmental factors, and political and personal circumstances (e.g., human rights violations, interpersonal violence). Forced migrants are particularly likely to have experienced traumatic events at this stage, which may affect their psychological and physical health status throughout their journey. An individual's health status also frequently reflects health policies and the strength of the health sector, including health promotion, service quality, and access. Policy dialogues related to pre-departure locations have focused primarily on screening for communicable diseases [23],[24] and the depletion of health care professionals from resource-poor areas [25], with less attention to, for example, the health of the elderly and children who are left behind [26],[27]. Although this is a beneficial time to conduct health promotion and offer information to potential migrants about health in the destination location, there has been little collaboration between countries of origin and destination. However, several countries with large numbers of labor migrants have begun to develop programs to inform individuals about health risks and service rights [28],[29] and have implemented multilateral employment and social insurance schemes with recruitment agencies and with destination countries [30],[31] (examples in Table 2).
Travel Phase
The travel phase encompasses the period when individuals are between their place of origin and a destination or an interception location. This phase might include multiple “transit” locations where individuals stop for short or long periods. From a global public health perspective, this is the stage during which pathogens may be carried across different zones of disease prevalence and initiate changes in international and local transmissible disease epidemiology. Travel restrictions have been a focus of attention after the recent outbreaks of pandemic influenza, even if there is limited evidence about their effectiveness [32],[33]. Especially for irregular migrants, health influences during this time are closely related to the mode of transport and circumstances of travel, such as journeys via flimsy boats or closed containers [34]. There are regular reports of Mexican migrants who die from heat exposure on treks across the desert towards the United States, or Burmese refugees fleeing through malaria-endemic areas [35],[36]. In cases of human trafficking, this phase is generally the time when criminal acts begin, such as illegal border crossings, kidnapping, and, for women and children, sexual violence. Evidence on health promotion programs at border or transit locations for migrants is scant. However, several health education and support initiatives have been established, for example, in US–Mexico border towns [37].
Destination Phase
The destination phase is when individuals settle either temporarily or long-term in their intended location. A majority of migration health research and policy attention has focused on this phase, usually describing issues in high-income and migrant-receiving countries and frequently investigating specific diseases, certain ethnic groups, or “the healthy migrant effect” [38]. However, greater attention is required for non-communicable diseases, mental health, and socioeconomic influences on health. Risk behaviors among migrants appear to change when they are in new settings such as when Japanese migrants to the US showed that as cultural adaptation became more pronounced, the risk of coronary heart disease began to match that of the host population [39]. Mental health outcomes often appear worse for migrants, displaced populations, and refugees than for native-born populations [40]. Migrant women may be at greater risk of reproductive health problems and poor pregnancy outcomes, such as pregnancy complications, neonatal morbidity, and infant mortality [41]. Asylum-seekers with temporary protection tend to have poorer mental health than refugees who have permanent residency [42] and similarly, low-skilled migrant laborers, especially those with irregular status, are at high risk of injury and illness [43].
Interception Phase
The interception phase applies to a small but particularly at-risk portion of the migrating population. This phase is characterized by situations of temporary detention or interim residence and is primarily relevant for forced migrants (e.g., asylum-seekers, refugees, displaced populations, trafficked persons) or irregular migrants, such as undocumented workers. Interception strategies for international migrants or displaced persons are frequently linked to immigration control policies and often have negative or punitive implications. Immigration detention centers or refugee camps often have deleterious effects on mental or physical health and are commonly sites of human rights abuses. There are clear associations between the length of detention and severity of mental disorders, especially for individuals with prior exposure to traumatic events, which is common among forced migrants. To date, few policy-level mandates have incorporated explicit measures to detect or prevent psychological morbidity in detention situations [44],[45]. In addition, detention conditions may be unhygienic or unsafe (particularly for women) [46],[47]. In high-resource settings, medical care for migrants in detention may be more advanced than in an individual's home country, but poorer compared to services available to the host population due to policies that, either by design or neglect, permit unequal treatment of migrants. Complex humanitarian emergency responses may be associated with the emergence of public health hazards by linking populations with disparate disease prevalence, but may also give rise to health-promoting measures, such as access to modern medical interventions and social services [48] and targeted prevention or treatment programs [49].
Return Phase
The return phase is when individuals go back to their place of origin, either temporarily or to resettle indefinitely or permanently. In this phase, vulnerable migrants may experience the cumulative toll that migration exposures have taken on their physical and psychological well-being. In some settings, returning migrants, especially those who move from rural to urban areas, may be responsible for introducing new pathogens or increasing the prevalence of infections among the local population [50]. Individuals returning to low-resource settings with life-threatening, disabling, or chronic health concerns that require ongoing or high-tech treatment, such as cancer, diabetes, or HIV, may have difficulty identifying or paying for adequate care. People who return after suffering serious abuse, such as trafficked persons or war-affected refugees, may sustain high levels of distress or psychiatric morbidity [51],[52]. Practices related to the repatriation of individuals with life-threatening conditions do not always fully adhere to human rights principles and can put returnees at risk of long-term morbidity or mortality [53],[54]. Particularly in post-conflict situations when refugees are resettled to locations that have been ravaged by war, highly vulnerable individuals are likely to encounter a dearth of necessary services [55]. Many labor migrants, however, may return with reasonable remuneration and remittances that help them afford a healthier lifestyle and better health care for themselves and their family. There is a need for bilateral or regional agreements to support the portability of health care benefits, especially when healthy migrants contribute to wealthy countries and return unwell or to retire and require significant care from their home country's health system [56].
Migration Health Policy Standards and Instruments
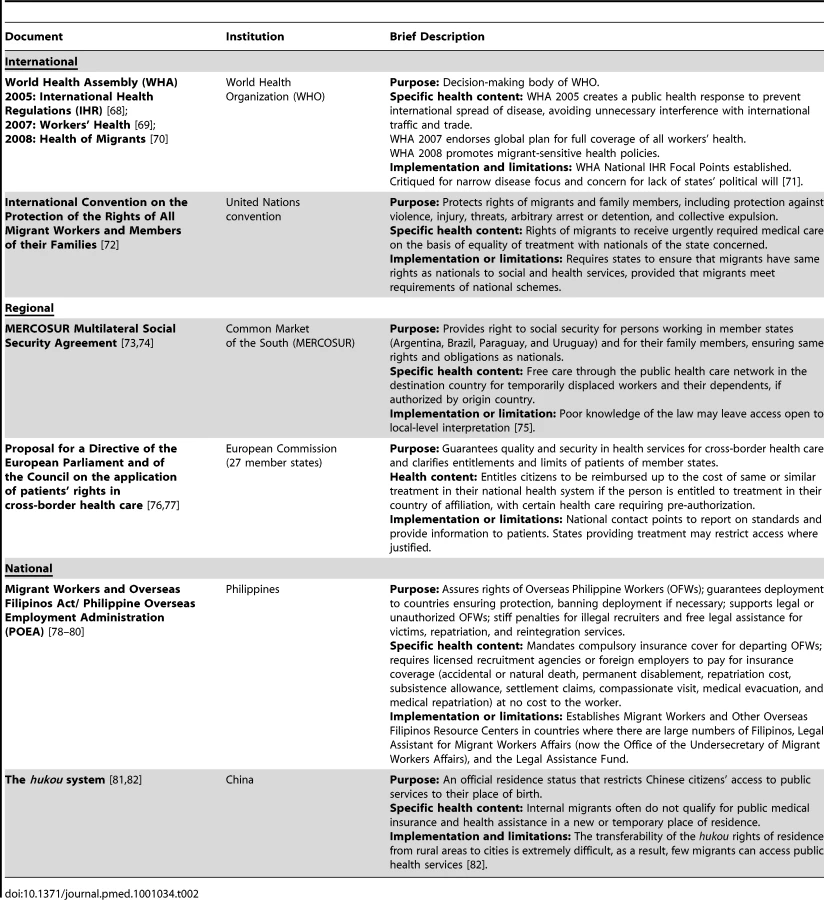
Table 2 presents examples of international instruments and regional and national legislation or policies related to health and migration. At the international level, the 61st World Health Assembly adopted a resolution that encouraged states to develop migrant-sensitive health policies and practices. The selected regional and national examples indicate the somewhat disjointed, sometimes conflicting, nature of migration health policy-making, as well as important gaps [57]. For instance, migrant health insurance schemes may be encumbered by restrictive immigration legislation or exclude undocumented migrants and migrants' family members from coverage. Similarly, regional agreements or national plans may promote economic cooperation through labor migration, but may not include portable health benefits. In practice, responsibility for fair health policies for migrants still lies within each nation state. And, even where multilateral agreements exist, their implementation does not automatically translate into universal, equal health opportunities for migrants.
Conclusions
If internal and international migrants compris`ed a nation, it would be the third most populous country in the world, just after China and India. Yet, attention to the health of migrants is still limited. Where migration health policies exist, they operate primarily in isolation at national levels and cover only fragmented snapshots of people's movement, with few binding regional or global health protection agreements to respond to the true scope of contemporary migration [7],[8].
Moreover, the chasm between practice and policy—those providing health services to migrants versus those making policies about migrants' entitlements—is increasingly evident. At the same time that clinicians are treating more diverse migrant groups, policy-makers are attempting to implement restrictive or exclusive immigration-related health policies that contradict public health needs and undermine medical ethics that operate on the ground.
Policies that respond to the diversity of migrant groups and their differential health risks and service access must be developed and implemented. Moreover, to make real advances in the protection of both individual and public health, interventions must target each stage of the migration process and reach across borders. Services should be based on human rights principles that foster available and accessible care for individual migrants.
Migration policy-making is wholly compatible with health-promoting strategies for migrants. As globalization appears to be irreversibly linked to population mobility and individuals have proven that they will continue to migrate and re-migrate, it is time for decision-makers from the migration and health sectors to sit at the same table with policy-makers from other sectors, such as development, humanitarian aid, human rights, and labor, to make migration safe and healthy for all.
Zdroje
1. United Nations Development Programme (UNDP) 2009 Human development report 2009: overcoming barriers: Human mobility and development New York UNDP
2. United Nations Department of Economic and Social Affairs Population DivisionUnited Nations, editor 2009 International migration 2009. New York UNDESA
3. United Nations Population Division 2009 International migrant stock: the 2008 revision Geneva United Nations Population Division
4. CastlesS 2000 International migration at the beginning of the 21st century: global trends and issues Paris UNESCO
5. GushulakBWeekersJMacPhersonD 2009 Migrants and emerging health issues in a globalized world—health threats, risks and challenges: an evidence-based framework. Emerging Health Threats Journal 2 e10 doi:10.3134/ehtj.09.010
6. StucklerDMcKeeM 2008 Five metaphors about global-health policy. Lancet 372 95 97
7. PacePGushulakB 2010 Policy and legal framework affecting migrants' health. Global consultation on migrant health; National School of Public Health; Madrid, Spain; 3N5 March 2010 Geneva WHO/Government of Spain/IOM
8. BettsA 2010 Migration governance: alternative futures Geneva IOM
9. World Health Organization 2010 Health of migrants–the way forward. Report of a global consultation Geneva World Health Organization
10. FortierJP World Health Organization, editor 2010 Migrant-sensitive health systems. Health of migrants - the way forward. Report of a global consultation Madrid WHO
11. UNAIDS 2009 Background paper: people on the move – forced displacement and migrant populations. 24th Programme Coordinating Board Thematic Segment Geneva UNAIDS
12. DaviesAABastenAFrattiniC 2009 Migration. A social determinant of the health of migrants. Eurohealth 16 10 14
13. LeeE 1966 A theory of migration. Demography 3 47 57
14. MasseyDArangoJHugoGKouaouciAPellegrinoA 1993 Theories of international migration: a review and appraisal. Population and Development Review 19 431 457
15. BellM 2004 Measuring temporary mobility: dimensions and issues Queensland Queensland Centre for Population Research School of Geography
16. PiperN 2003 Feminization of labor migration as violence against women. International, regional, and local nongovernmental organization responses in Asia. Violence Against Women 9 723 745
17. PessarPR Department of Economic and Social Affairs, United Nations Secretariat, editor 2005 Women, gender and international migration across and beyond the Americas. Inequalities and limited empowerment. Expert group meeting on international migration and development in Latin America and the Caribbean; 30 November–2 December 2005. UN/POP/EGM-MIG/2005/08 New York United Nations Secretariat
18. CrawleyHLesterT 2004 Comparative analysis of gender-related persecution in national asylum legislation and practice in Europe Geneva United Nations High Commissioner for Refugees
19. PaceP 2010 What can be done in EU Member States to better protect the health of migrants? Eurohealth 16 5 9
20. GushulakB 2000 Health determinants in migrants: the impact of population mobility on health. van KriekenPJ Health, migration and return: a handbook for a multidisciplinary approach The Hague Asser Press
21. ZimmermanCYunKWattsCShvabITrappolinL 2003 The health risks and consequences of trafficking in women and adolescents. Findings from a European study London London School of Hygiene & Tropical Medicine and the Daphne Programme of the European Commission
22. GushulakBDMacPhersonD 2000 Health issues associated with the smuggling and trafficking of migrants. J Immigr Health 2 67 78
23. KlinkenbergEManisseroDSemenzaJSSV 2009 Migrant tuberculosis screening in the EU/EEA: yield, coverage and limitations. Eur Respir J 34 1180 1189
24. WelshmanJBashfordA 2006 Tuberculosis, migration, and medical examination: lessons from history. J Epidemiol Community Health 60 282 284
25. AwasesMGbaryANyoniJChatoraR 2004 Migration of health professionals in six countries: a synthesis report Brazzaville (Republic of Congo) World Health Organization Regional Office for Africa 68
26. AbasMAPunpuingSJirapramukpitakTGuestPTangchonlatipK 2009 Rural–urban migration and depression in ageing family members left behind. Br J Psychiatry 195 54 60
27. ConnellJZurnPStilwellBAwasesMBraichetJ-M 2007 Sub-Saharan Africa: beyond the health worker migration crisis. Soc Sci Med 64 1876 1891
28. SiddiquiIRashidRZeitlynB 2008 Information campaigns on safe migration and pre-departure training Sussex Development Research Centre on Migration, Globalisation and Poverty
29. UNAIDS 2000 Regional Summit on pre-departure post arrival and reintegration programs for migrant workers Kuala Lumpur Caram Asia
30. Abdul-AzizA-R 2001 Bangladeshi migrant workers in Malaysia's construction sector. Asia-Pacific Population Journal 16 3 22
31. CarrasquilloOCarrasquilloAISheaS 2000 Health insurance coverage of immigrants living in the United States: differences by citizenship status and country of origin. Am J Public Health 96 917 923
32. FergusonNCummingsDFraserCCajkaJCooleyP 2006 Strategies for mitigating an influenza pandemic. Nature 442 448 452
33. EpsteinJGoedeckeDYuFMorrisRWagenerD 2007 Controlling pandemic flu: the value of international air travel restrictions. PLoS ONE 2 e401 doi:10.1371/journal.pone.0000401
34. [No authors listed] 16 December 2010 Boat people in Australia - asylum or death? The tragic sinking revives a debate about boat people. The Economist London The Economist Newspaper Limited Available: http://www.economist.com/node/17733127?story_id=17733127&fsrc=rss. Accessed 25 April 2011
35. SapkotaSKohlHWGilchristJMcAuliffeJParksB 2006 Unauthorized border crossings and migrant deaths: Arizona, New Mexico, and El Paso, Texas, 2002–2003. Am J Public Health 96 1282 1287
36. RowlandMNostenF 2001 Malaria epidemiology and control in refugee camps and complex emergencies. Ann Trop Med Parasitol 95 741 754
37. Forster-CoxSMangaduTJacquezBFullertonL 2010 The Environmental Health/Home Safety Education Project: a successful and practical U.S.-Mexico border initiative. Health Promot Pract 11 325 331
38. NewboldB 2005 Self-rated health within the Canadian immigrant population: risk and the healthy immigrant effect. Soc Sci Med 60 1359 1370
39. MarmotMGSymeSL 1976 Acculturation and coronary heart disease in Japanese-Americans. Am J Epidemiol 104 225 247
40. SteelZCheyTSiloveDMarnaneCBryantRA 2009 Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: a systematic review and meta-analysis. JAMA 302 537 549
41. BolliniPPampallonaSWannerPKupelnickB 2009 Pregnancy outcome of migrant women and integration policy: a systematic review of the international literature. Soc Sci Med 68 452 461
42. MomartinSSteelZCoelloMArocheJSiloveD 2006 A comparison of the mental health of refugees with temporary versus permanent protection visas. Med J Aust 185 357 361
43. AhonenEQBenavidesFGBenachJ 2007 Immigrant populations, work and health–a systematic literature review. Scand J Work Environ Health 33 96 104
44. SteelZSiloveDBrooksRMomartinShakehAlzuhairiB 2006 Impact of immigration detention and temporary protection on themental health of refugees. Br J Psychiatry 188 58 64
45. KellerARosenfeldBTrinh-ShevrinCMeserveCSachsE 2003 Mental health of detained asylum seekers. Lancet 362 1721 1723
46. SiloveDSteelZMollicaRF 2001 Refugees - detention of asylum seekers: assault on health, human rights, and social development. Lancet 357 1436 1437
47. Mekong Migration Network (MMN) 2009 Death of 2 Burmese indicative of state of detention places in Malaysia. Denial of healthcare is a violation of right to life. Joint statement on behalf of 123 organizations/groups. Chiang Mai: MMN
48. KimGTorbayRLawryL 2007 Basic health, women's health, and mental health among internally displaced persons in Nyala Province, South Darfur, Sudan. Am J Public Health 97 353 361
49. LegrosDPaquetCPereaWMartyIKenya MugishaN 1999 Mass vaccination with a two-dose oral cholera vaccine in a refugee camp. Bull World Health Organ 77 873 842
50. LurieMNWilliamsBGZumaKMwamburiDMGarnettGP 2003 The impact of migration on HIV-1 Transmission in South Africa. A study of migrant and nonmigrant men and their partners. Sex Transm Dis 30 149 156
51. HossainMZimmermanCAbasMLightMWattsC 2010 The relationship of trauma to mental disorders among trafficked and sexually exploited girls and women. Am J Public Health 100 2442 2449
52. FuHVanLandinghamMJ 2008-07 Mental and physical health consequences of repatriation for Vietnamese returnees: a natural experiment approach New Orleans Department of International Health and Development, School of Public Health and Tropical Medicine, Tulane University
53. [No authors listed] 2010 The UK's continued shameful neglect of migrants' health. The Lancet 376 1438
54. TravisA 16 January 2008 Immigration chief defends deportation of cancer patient. The Guardian. London. Available: http://www.guardian.co.uk/uk/2008/jan/16/immigration.politics. Accessed 25 April 2011
55. SinghKKarunakaraUBurnhamGHillK 2005 Forced migration and under-five mortality: a comparison of refugees and hosts in North-western Uganda and Southern Sudan. European Journal of Population/Revue européenne de Démographie 21 247 270
56. HolzmannRKoettlJChernetskyT 2005 Portability of pension and health care benefits for international migrants: an analysis of issues and good practices Washington (D.C.) The World Bank
57. World Health AssemblyWorld Health Assembly, editor. 2008 Health of migrants. Executive Board Resolution. 122R5 Geneva World Health Assembly
58. UNESCO 2011 Social and human sciences: international migration - glossary of migration related terms Paris UNESCO Social and Human Sciences
59. PortesABoroczJ 1989 Contemporary immigration: theoretical perspectives on its determinants and modes of incorporation. Int Migr Rev 23 606 630
60. United Nations 2000 Protocol to prevent, suppress and punish trafficking in persons, especially women and children, supplementing the United Nations Convention against transnational organized crime Vienna UNODC
61. UN General Assembly 1990 International Convention on the Protection of the Rights of All Migrant Workers and Members of Their Families. G.A. res. 45/158, annex, 45. U.N. GAOR Supp. (No. 49A) at 262, U.N. Doc. A/45/49 (1990), entered into force 1 July 2003
62. International Labour Organization (ILO) 2009 Database on international labour migration statistics (ILM) Geneva ILO
63. UNHCR 2010 UNHCR statistical online population database Geneva UNHCR
64. UN General Assembly 1951 Convention and Protocol Relating to the Status of Refugees Geneva UNHCR
65. United Nations World Tourism Organization (UNWTO) 2009 UNWTO tourism highlights Madrid UNWTO
66. United Nations 1998 Recommendations on statisitcs of international migration - revision 1 New York Department of Economic and Social Affairs, Statistics Division
67. UNESCO Institute for Statistics 2010 Statistics data centre Monteal UNESCO
68. World Health OrganizationWorld Health Organization, editor 2008 International Health Regulations 2005. 2nd edition Geneva WHO 74
69. Sixtieth World Health AssemblyWorld Health Organization, editor 2007 Workers' health: global plan of action. Geneva WHO
70. Sixty-First World Health AssemblyWorld Health Organization, editor 2008 Health of migrants. Geneva WHO
71. FidlerDGostinL 2006 The new International Health Regulations: an historic development for international law and public health. J Law Med Ethics 85 94
72. UN General Assembly 1990 UN General Assembly GA, annex, 45. GAOR Supp. (No. 49A) at 262, U.N., entered into force 1 July (18 December 1990). International Convention on the Protection of the Rights of All Migrant Workers and Members of Their Families
73. CabanasM 2009 The MERCOSUR Multilateral Social Security Agreement. Seguridad Social 257 57 71
74. Supremo Tribunal de Justica da Republica Federativa do Brasil 1997 Acordo Multilateral de Seguridade Social do Mercado Comum do Sul. Norma da Corte Suprema. Montevideo
75. GiovanellaLGuimaraesLNogueiraVLobatoLDamacenaG 2007 Health on the borders: access to and demands on the Brazilian National Health System by foreigner and non-residents of Brazilians in cities along the border with MERCOSUR countries from the perspective of municipal health secretaries. Cad Saude Publica 23 S251 S266
76. Legido-QuigleyHPassaraniIKnaiCBusseRPalmW 2011 Cross-border healthcare in the European Union: clarifying patients' rights. BMJ 342 d296
77. Commission of the European CommunitiesCommission of the European Communities, editor 2008 Proposal for a Directive of the European Parliament and of the Council on the application of patients' rights in cross-border healthcare. 2008/0142 Brussels 414
78. President of the Philippines 1987 Reorganizing the Philippine Overseas Employment Administration and for other purposes. Executive Order No 247. Manilla
79. President of the Philippines 1982 Reorganizing the Ministry of Labor and Employment, creating the Philippine Overseas Employment Administration and for other purposes. Executive Order No 797. Manilla
80. Senate and House of Representatives of the Philippines 1995 Migrant Workers and Overseas Filipinos Act of 1995
81. HuXCookSSalazarM 2008 Internal migration and health in China. Lancet 327 1717 1719
82. TodrysKAmonJ 2009 Within but without: human rights and access to HIV prevention and treatment for internal migrants. Global Health 2009 1 17
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2011 Číslo 5
- Alternativní léčebné možnosti u hypercholesterolemie při intoleranci statinů
- Vliv kombinace nutraceutik na remodelaci levé komory srdeční u osob s metabolickým syndromem
- Nutraceutika a jejich ovlivnění mírného kardiometabolického rizika
- Princip účinku medu v léčbě chronických i infikovaných ran
- Superoxidovaný roztok a jeho využití v léčbě ran
Nejčtenější v tomto čísle
- Low-Dose Adrenaline, Promethazine, and Hydrocortisone in the Prevention of Acute Adverse Reactions to Antivenom following Snakebite: A Randomised, Double-Blind, Placebo-Controlled Trial
- Effectiveness of Early Antiretroviral Therapy Initiation to Improve Survival among HIV-Infected Adults with Tuberculosis: A Retrospective Cohort Study
- Medical Students' Exposure to and Attitudes about the Pharmaceutical Industry: A Systematic Review
- Estimates of Outcomes Up to Ten Years after Stroke: Analysis from the Prospective South London Stroke Register