
Assessing the neuroprotective benefits for babies of antenatal magnesium sulphate: An individual participant data meta-analysis
In an individual participant data meta-analysis, Caroline Crowther and colleagues examine the evidence for the neuroprotective benefits of antenatal magnesium sulphate for babies.
Published in the journal:
. PLoS Med 14(10): e32767. doi:10.1371/journal.pmed.1002398
Category:
Research Article
doi:
https://doi.org/10.1371/journal.pmed.1002398
Summary
In an individual participant data meta-analysis, Caroline Crowther and colleagues examine the evidence for the neuroprotective benefits of antenatal magnesium sulphate for babies.
Introduction
Worldwide, each year, almost 15 million babies are born preterm (before 37 completed weeks of gestation)—11% of all births [1]. Babies born preterm are at greater risk of dying in early life compared with those born at term [2,3]. Preterm babies who survive have a higher risk for neurologic impairments, such as cerebral palsy, blindness, deafness, or cognitive dysfunction, and, as a result, are at greater risk of substantial disability [4]. The earlier the gestation at birth is, the greater these risks become. Global estimates suggest that up to 8% of preterm babies have neurological impairments, of which 5% are mild and 3% moderate or severe [5]. Cerebral palsy and cognitive dysfunction, either intellectual impairment or developmental delay, are the most frequent cause of neurological impairment. With the rate of preterm birth increasing in many countries, more babies are at risk of dying and, among those who survive, of having an adverse neurological outcome, making the global burden substantial [6]. Effective therapies that can reduce the risk of neurological impairments and disabilities for preterm survivors are urgently needed.
The linkage of antenatal magnesium sulphate to a reduction in cerebral palsy arose from seminal observational studies in the mid-1990s [7,8]. Several randomised trials followed, the latest reported in 2008 [9,10,11,12,13]. When the Cochrane review assessing the use of magnesium sulphate for women at risk of preterm birth for neuroprotection of the fetus was updated in 2009 [14], for the first time, a clinically important reduction in the risk of cerebral palsy was identified using aggregate data meta-analysis methods. There was a relative risk reduction of nearly a third in cerebral palsy (32%) in children born to women allocated magnesium sulphate prior to preterm birth compared with controls. Although the absolute risk reduction of 1.7% for cerebral palsy was small, it represented a huge advance in minimising a burden of illness that has so far proved very resistant to intervention. The exact mechanism by which magnesium exerts a neuroprotective effect is unclear. Magnesium sulphate can block cerebral glutamate receptors, and this may prevent posthypoxic brain injury in the perinatal period [14].
The Cochrane review was unable to provide some details needed by guideline developers, policy makers, clinicians, and pregnant women—notably, whether antenatal magnesium sulphate treatment is more effective in some women by reason of their risk of preterm birth, what the gestational age range is for maximal benefit, what dose and timing prior to birth is best, and whether maintenance treatment or retreatment is necessary [15,16]. The AMICABLE (Antenatal magnesium sulphate individual participant data international collaboration: Assessing the benefits for babies using the best level of evidence) Group was formed to undertake a meta-analysis of the individual participant data of the eligible trials. The advantages of individual participant data meta-analysis (IPD-MA) for exploring interactions between treatment and participant-level characteristics and enabling examination of differential treatment effects between subgroups are well described [17,18,19]. The objectives of the AMICABLE IPD-MA were to assess, using IPD methods and meta-analyses, the effects of administration of antenatal magnesium sulphate given to women at risk of preterm birth on important clinical outcomes.
Methods
The Children, Youth and Women’s Health Service Research Ethics Committee, South Australia, Australia, approved the study (REC2315/10/13). The included trials had received country-specific ethical review, with individual participants providing written, informed consent. The IPD meta-analysis followed the published protocol (S2 Text) [20], and the results are reported using the Preferred Reporting Items for Systematic Review and Meta-analyses of Individual Participant Data (PRISMA-IPD Statement) checklist (S1 Text) [21].
Specific objectives
The specific objectives of the AMICABLE IPD-MA were to assess whether the treatment effects of antenatal magnesium sulphate given to women at risk of preterm birth differ depending on the following important prespecified participant and treatment characteristics [20]:
the reason the woman was considered to be at risk of preterm birth (such as preterm labour, hypertensive disease of pregnancy, antepartum haemorrhage, or presence of ruptured membranes);
the primary reason antenatal magnesium sulphate treatment was given (such as neuroprotection of the fetus, pre-eclampsia, or tocolysis);
the number of babies in utero (singleton or multiple);
the gestational age at which antenatal magnesium sulphate treatment was given;
the time prior to birth when antenatal magnesium sulphate treatment was given;
the type, mode of administration, and dosage of antenatal magnesium sulphate planned and given;
whether maintenance treatment with antenatal magnesium sulphate was planned and used; and
whether repeat antenatal magnesium sulphate treatment was planned and used.
Eligibility criteria
Trials in which women considered at raised risk of preterm birth (less than 37 weeks' gestation) were randomised to either magnesium sulphate or no treatment were considered eligible. Trials were included if the primary aim of the study was to prevent neurologic abnormalities in the unborn baby or if the primary aim was otherwise but early childhood neurological outcomes were reported for the infants. Quasirandom study designs were not eligible.
Identifying studies: Information sources and search strategy
The search strategy developed by the Cochrane Pregnancy and Childbirth Group [22] was used. This identified trials from monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL); weekly searches of MEDLINE; monthly searches of CINAHL (EBSCO); hand-searches of 30 journals and the proceedings of major conferences; and weekly current awareness alerts for a further 44 journals, plus monthly BioMed Central email alerts.
Searches used the terms [antenatal or prenatal] and [magnesium] and [preterm or premature or neuroprotection or 'cerebral palsy']. The date of the last search was 28 February 2017. In addition, the World Health Organisation (WHO)/CTRP portal was accessed to identify any recently completed or ongoing trials. The date of the last search was 3 May 2017. There was no language restriction on the searches. Trialists within the AMICABLE Group were asked if they knew of any unpublished or other trials.
Study selection processes
Eligibility for inclusion of the identified trials was assessed independently by 2 unblinded members of the AMICABLE Project Team (PFM and TKB). Any differences in opinion regarding eligibility were resolved by discussion. For the MAGPIE Trial [12], the primary aim of the study was neuroprotection of the mother with pre-eclampsia rather than neuroprotection of the fetus. Childhood neurological outcomes were available from centres selected for longer-term follow-up. Data were included from participants in the longer-term follow-up who were preterm at trial entry (<37 weeks’ gestation).
Data collection processes and data items
The chair of the AMICABLE Project Team contacted the investigators of all eligible studies to invite them to join the AMICABLE Trialist Group and to include IPD from their trial in the meta-analysis.
Prespecified and clearly defined variables (both for participant-level and trial-level factors as well as for outcomes) were identified and confirmed by the AMICABLE Trialist Group. Investigators were asked whether these variables had been collected or could be derived for their study. A coding system was developed from these variables.
Deidentified data were collected on all women randomised. These included baseline data for descriptive purposes and analyses (reason at raised risk of preterm birth, gestational age at trial entry, plurality of the pregnancy, and expected date of birth) and details of the intervention planned and given (the date of randomisation, the allocated intervention, the type and dose of magnesium sulphate given, the mode of administration, whether a maintenance dose was given, and whether retreatment was given and its amount), together with the maternal and infant outcomes to allow the planned analyses.
The individual trial data were recoded as required and stored in a custom-designed secure database only accessible by authorised personnel from the AMICABLE Data Management Group. Trialists from the individual trials were asked to verify their own coded data prior to the analyses.
Data were checked with respect to range, internal consistency, missing or extreme values, errors, and consistency with the published reports. Trial details such as randomisation methods and intervention details were cross-checked against trial protocols, clinical record forms, and published reports. The AMICABLE biostatistician, project, and data managers liaised closely with the investigators from the individual trials to clarify any inconsistencies and missing data. Each trial was analysed individually, and the final IPD dataset generated for each trial was sent to the appropriate trial investigator for verification before synthesising into the full AMICABLE dataset. Data items collected are published elsewhere (S3 Text) [20].
IPD integrity
Risk of bias assessment in individual studies
Using the Cochrane Collaboration risk of bias tool [23], the risk of bias for each study was assessed independently by 2 members of the AMICABLE Project Team (PFM and TKB), with differences resolved by discussion. Each study was judged to have a high, low, or unclear risk of bias for random sequence generation (checking for possible selection bias), allocation concealment (checking for possible selection bias), blinding of participants and personnel (checking for possible performance bias), blinding of outcome assessment (checking for possible detection bias), incomplete outcome data (checking for possible attrition bias due to the amount, nature, and handling of incomplete outcome data), selective reporting (checking for reporting bias), and other bias (checking for bias due to problems not already covered). The magnitude and direction of the bias and whether it was considered likely to affect the findings were assessed. Additional information was sought from the trialists if any aspect was unclear.
Specification of outcomes and effect measures
The 2 primary prespecified outcomes were a composite of death (defined as any fetal death after randomisation or death of a live-born infant before follow-up) or cerebral palsy for the infant (as defined by the trialists and categorised as mild, moderate, or severe) and, for the mother, any severe maternal outcome potentially related to treatment (defined as death, respiratory arrest, or cardiac arrest). Secondary outcomes were prespecified in the protocol (S4 Text) [20].
Synthesis methods
A detailed statistical analysis plan was prepared by the AMICABLE Data Management Group and agreed upon by the AMICABLE Trialist Group prior to the data analyses. All analyses were based on the checked and updated IPD from all trials. All randomised participants with outcome data available were included in the analyses, which were performed on an intention-to-treat basis, according to the treatment allocation at randomisation. No changes were made to the prespecified analysis plan. Further description of the statistical methods is included in the protocol [20].
For each of the outcomes, a 1-stage approach to analysis was taken so that the IPD from all eligible trials were included in a single model. Fitting a single model for each outcome variable enabled the variation across trials to be accounted for within the model. A treatment-by-trial interaction term was tested to assess heterogeneity of treatment effect across trials. If there was excessive statistical heterogeneity in the treatment effect across trials (i.e., the trial-by-treatment interaction term was significant), then the rationale for combining trials was questioned and the source of heterogeneity explored.
Binary outcomes were analysed using log-binomial regression models, and the results are presented as relative risk RR) with 95% confidence intervals (CIs) and associated 2-sided p-values. Continuous outcomes were analysed using linear regression models, and the results are presented as differences in means with 95% CIs and 2-sided p-values. Correlations between outcomes due to multiple births were taken into account using generalised estimating equations (GEEs), when appropriate.
Any differences in treatment effect between prespecified subgroups were assessed by testing a treatment by subgroup interaction term within the model. If data were missing for an outcome, those participants were removed from the analysis for that outcome. Reasons for missingness were explored, when possible. For each outcome, if there were unbalanced or large amounts of missing endpoint data for at least 1 trial, then sensitivity analyses were undertaken to assess the impact of removing such trials from the analysis.
Categorical outcomes were analysed using proportional odds models. Analyses of raw growth measurements (head circumference, weight, and length) were adjusted for age corrected for prematurity and sex, and analyses of WHO calculated z-scores of growth measurements were unadjusted for age and sex.
Missing data were accounted for in the following 2 ways. The main method for accounting for missing data for binary outcomes was to assume that participants with no data for that outcome did not have the outcome. This is referred to as the ‘Impute “No”‘ method.
Secondly, for the primary outcome (death or CP) missing CP values at follow-up were imputed using multiple imputations (MIs). One hundred MI datasets were imputed using the Stata version 11.2 ‘ice’ (MI using chained equations) function. Counts and percentages within each treatment group for MI analyses represent average percentages in the imputed datasets. Trial-specific estimates and standard errors for imputed analyses are from MI GEE models adjusting for correlation between multiple births. Overall relative risk estimates for meta-analyses containing results from the MI models were calculated using a 2-stage aggregate meta-analysis approach with inverse variance weighting.
The following sensitivity analyses were conducted:
exclusion of trials that were not for the purpose of neuroprotection of the fetus
exclusion of trials with high rates of participant exclusions, where losses were considered to have the potential to affect the results.
Results
Study characteristics
Seven randomised trials were identified through database searching [9,10,11,12,13,24,25], 2 of which were ongoing randomised trials [24,25]. Five randomised controlled trials were identified from the search, and each contributed data for the IPD meta-analyses (Fig 1) [9,10,11,12,13]. Details of the studies are described in Table 1.


IPD integrity
Overall, the risk of bias was low in the included studies, with some variation between trials (Table 2).

Risk of bias across studies
There was a generally low risk of bias across the studies, except for 3 of the 5 studies in which the risk of bias associated with attrition was rated as unclear.
Primary outcomes
A. Death or cerebral palsy
There was no statistically significant effect of antenatal treatment with magnesium sulphate on the composite outcome death or cerebral palsy in infants in the combined analyses (Table 3).

In the prespecified sensitivity analysis of the 4 trials with fetal neuroprotective intent, there was a statistically significant reduction in the risk of death or cerebral palsy (Table 4) with no significant heterogeneity (p = 0.28). The number needed to treat (NNT) to benefit was 41 women/babies to prevent 1 baby from either dying or having cerebral palsy (CP).

B. Severe adverse maternal events related to treatment
There were no events for the primary outcome of severe adverse maternal events related to treatment (including death or respiratory or cardiac arrest) and, accordingly, no events for maternal death or for severe maternal adverse events reported separately (total of 1,635 women: [9,10]).
C. Paediatric mortality
For the primary paediatric outcome of mortality, the overall mortality rates were 14.3% for babies exposed to magnesium sulphate and 13.6% for those exposed to the control treatment, not a statistically significant effect (Table 5).

D. Cerebral palsy
There was a strong protective effect of magnesium sulphate on the rate of CP, both for all studies (NNT to benefit 46 babies) (Table 6) and for the analysis limited to the fetal neuroprotective studies only (NNT to benefit 42 babies) (Table 7).


Overall, there were significant reductions in the rates of both moderate and severe CP combined (event rates 2.12% MgSO4, 3.36% controls; RR 0.63, 95% CI 0.44 to 0.90) and severe CP alone (event rates 0.81% MgSO4, 1.50% controls; RR 0.54, 95% CI 0.30 to 0.94), with no significant heterogeneity among trials for either outcome.
Maternal secondary outcomes
Of the maternal secondary outcomes, the only statistically significant effect was an increase in adverse events leading to stopping treatment in the magnesium sulphate group (Table 8). There were no clear differences in infectious morbidity (19.1% magnesium sulphate versus 18.8% control), mode of birth by caesarean (48% versus 46.3%), or postpartum haemorrhage (28.1% versus 28.1%).

Neonatal secondary outcomes
No statistically significant differences or any significant heterogeneity were seen in any of the analyses for the other neonatal morbidity dichotomous outcomes reported or defined by the trialists, including Apgar score at 5 minutes < 7, active resuscitation at birth, use of ongoing respiratory support after birth, any intraventricular haemorrhage (IVH), severe IVH (grade 3 or 4), cystic periventricular leucomalacia (PVL), neonatal convulsions, neonatal encephalopathy, chronic lung disease/bronchopulmonary dysplasia (BPD), posthaemorrhagic hydrocephalus or ventriculomegaly, proven systemic infection, necrotising enterocolitis (NEC), patent ductus arteriosus (PDA) requiring treatment, any retinopathy of prematurity (ROP), or severe neonatal adverse outcome (death, BPD, PDA, NEC, stage 3 or worse ROP, or grade 3 or 4 IVH); or the continuous outcomes (weight, head circumference, or length at birth) (Table 9). There was, however, a slightly lower birthweight z-score (mean difference −0.05, 95% CI −0.10 to −0.00; p = 0.04), a result obtained with no significant heterogeneity among the trials (p = 0.82) (Table 9).

Paediatric secondary outcomes
The meta-analysis found no evidence of statistically significant differences or significant heterogeneity for any of the analyses for the follow-up outcomes reported or defined by the trialists. Of note, weight z-scores at follow-up did not clearly differ between groups (Table 10).

Subgroup analyses
As there were no events, the planned subgroup analyses for severe maternal adverse outcomes potentially related to treatment were not possible. Not all trials had data available to contribute to all subgroup analyses.
A. Primary reason pregnancy was considered to be at raised risk of preterm birth
Among the 4 trials able to contribute data to this analysis, there were no clear differences in treatment effects among the subgroups considered by individual causes for the high-risk pregnancy (Table 11).

B. Purpose of treatment: Neuroprotection of the fetus versus other purpose
There was a significant difference in the magnitude of the treatment effect for death or CP for studies with the intent of fetal neuroprotection compared with studies with a different purpose. A significant reduction in death or CP was seen in the ‘neuroprotection’ group, but not in the ‘other’ reason group. There were no clear differences in treatment effects for the other outcomes (Table 12).

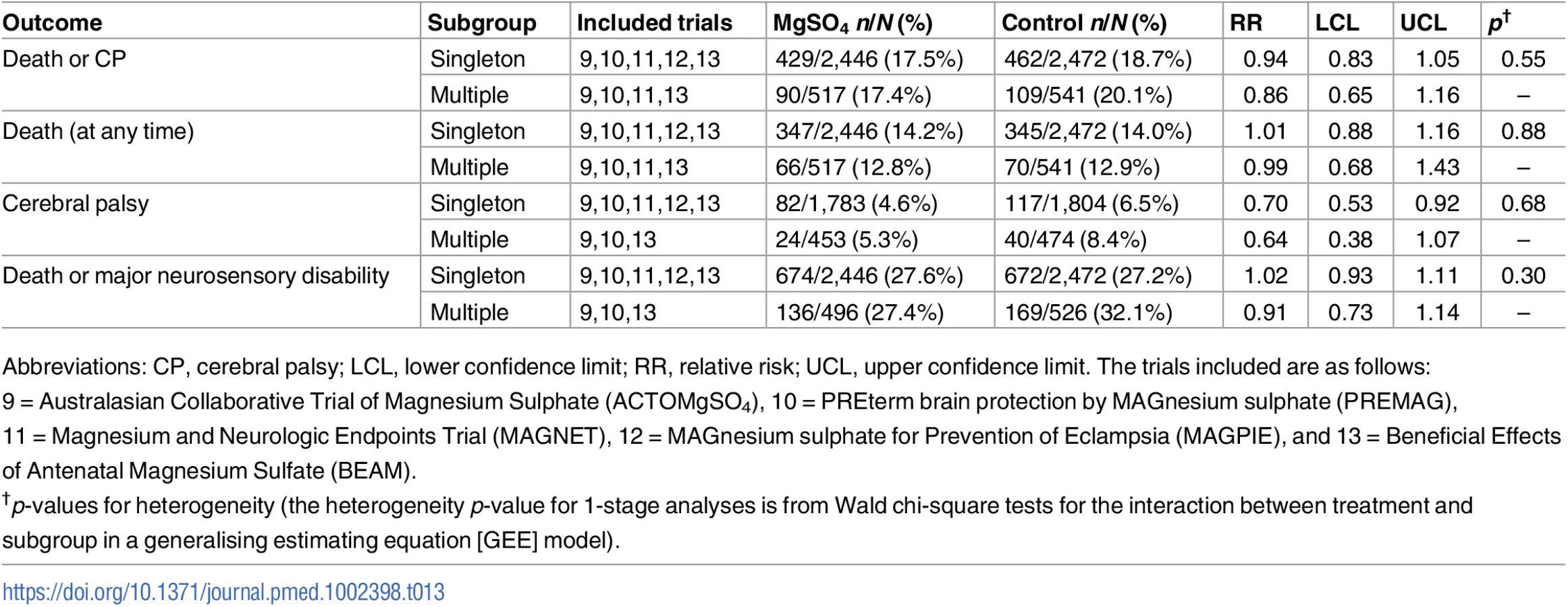
C. Multiple birth
There were no clear differences in treatment effects among the subgroups considered by multiple birth (Table 13).
D. Gestational age at randomisation
Inclusion criteria for gestational age at trial entry varied across trials. Several different, prespecified combinations of gestational age groupings were considered. No obvious monotonic trends were seen for any of the major outcomes when categorised by gestational age when first treated, and no statistically significant heterogeneity was observed among any subgroups (Table 14, S2 Table).

E. Time from first treatment until birth
Several different, prespecified combinations of time from first treatment to birth were considered. No obvious linear trends were seen for any of the major outcomes when categorised by time from when first treated until birth, and no significant heterogeneity was observed among any subgroups (Table 15 and S3 Table).

F. Total dose received
The total dose of MgSO4 received varied by trial because of different treatment protocols; therefore, the effect of increased dose on primary outcomes was explored. Several different, prespecified combinations of dosage groupings were considered. No obvious linear trends were seen for any of the major outcomes when categorised by dose received, and no significant heterogeneity was observed (Table 16 and S4 Table).

G. Maintenance therapy received
There were no clear differences in treatment effects among the subgroups considered by whether maintenance therapy had been received or not (Table 17).

H. Whether repeat antenatal magnesium sulphate treatment was received
No trial was able to provide data to contribute to this planned subgroup analysis.
Sensitivity analyses to account for missing data
Regardless of the methods used to account for missing data, no conclusions were altered compared with the main results reported above for any of the outcomes (S5 Table).
Discussion
Summary of evidence
The major finding from this IPD-MA is that for women at risk of imminent preterm birth antenatal, magnesium sulphate reduces the risk of their baby developing CP, with a NNT to benefit of 46 babies. The neuroprotective effect is confirmed when the primary reason for giving the antenatal magnesium sulphate is for neuroprotection of the fetus. Importantly, this benefit is not at the expense of an increase in mortality for the baby, and there appear to be no substantial short - or long-term complications for the mother or fetus from treatment with antenatal magnesium sulphate.
The results from this IPD-MA are consistent with the findings of the existing aggregate data meta-analysis in the Cochrane Library [14]. The new information that this IPD-MA has been able to clarify is that no particular subgroup of women and babies benefitted more or less from treatment among varying reasons for preterm birth, varying preterm gestational ages when treatment was started, or with varying dosage regimens, including whether maintenance therapy was given after a loading dose or not. Consequently, the information from the IPD-MA shows that there are no particular subgroups of women or their babies who might benefit more from treatment compared to others. The IPD-MA shows that antenatal magnesium sulphate reduces not only all CP, the majority of which is mild, but also moderate and severe combined and severe CP alone. Of note, the beneficial effect of magnesium sulphate on CP was not associated with fewer severe cerebral morbidities such as grade 3–4 intraventricular haemorrhage or cystic periventricular leucomalacia.
No severe adverse maternal events (including death or respiratory or cardiac arrest) were recorded for the 2 studies able to provide data for this IPD-MA. While reassuring, information about these rare maternal events should be routinely collected [26]. In combination with the known but less serious side effects of magnesium sulphate, such as flushing and tachycardia, the fact that maternal side effects are more likely to lead to stopping of a beneficial treatment than placebo and that severe maternal events are possible highlight the importance of giving magnesium sulphate under appropriate supervision [26,27].
The lack of an effect of magnesium sulphate on Apgar scores at 5 minutes, a need for active resuscitation at birth, or a need for ongoing assisted ventilation after birth indicates that magnesium sulphate, as used in these trials, does not have any substantial effect on depressing infant breathing after birth, either immediately or in the early hours and days of life, after which time the drug would usually have been excreted through the urinary system.
There were no substantial relationships between time from starting magnesium treatment until birth, the total dose received, or whether maintenance treatment was received and any of the major health outcomes. As these events all occur postrandomisation and therefore may be affected by the treatment given, interpretation of the results must be cautious. With maternal side effects increasing with higher total dose [26] and with concerns about maternal safety, at a clinical level it may be prudent to limit treatment to times close to birth and to minimise the dose of magnesium used to a 4-g bolus loading dose with or without a maintenance dose of 1 g/hour.
Strengths and limitations
IPD-MA is recognised as the gold standard for systematic reviews [17]. One of the strengths of this study is that we have been able to include individual participant data from all of the known completed randomised clinical trials of magnesium sulphate for which developmental outcomes for the child have been reported.
We are aware of 2 ongoing placebo-controlled trials of antenatal magnesium sulphate for neuroprotection of the fetus that will report on childhood development: one in women at risk of preterm birth from 24 to <32 weeks’ gestation with a sample size of 500 [24] that is due to report in 2018 and the other where preterm birth is expected or planned between 30 to <34 weeks’ gestation, with a planned sample size of 1,676 babies and expected to report in 2021 [25]. Ultimately, data from these trials will be eligible to contribute to an update of this IPD-MA.
The limitations of our study are that not all trials had collected or could provide the data required for all of the prespecified analyses. Given that maternal and fetal event rates are low for some important clinical events, the power to find any overall or subgroup differences was limited. Lack of data from individual studies compounded the problem of low power for some of the analyses. Several of the planned analyses were for events that occurred after randomisation, including total dose received and the duration between start of treatment and birth. We recognise that such events are more subject to bias, but our intent was to identify subgroups of mothers who benefitted most and thus enable use of antenatal magnesium sulphate therapy to be better targeted.
Conclusions
This IPD meta-analysis reaffirms that antenatal magnesium sulphate given prior to preterm birth is neuroprotective for CP and reduces the combined risk of fetal/infant death or CP, when the primary intent of magnesium sulphate treatment is fetal neuroprotection. Antenatal magnesium sulphate is a relatively inexpensive, easy to administer, effective treatment that can reduce the burden of death and CP facing babies born very preterm. Widespread adoption of the recommendations to use magnesium sulphate within several national clinical practice guidelines [15,16,28,29] and now within the recent WHO recommendations on interventions to improve preterm birth outcomes [3] could lead to significant global health benefits.
It is reassuring that antenatal magnesium sulphate does not appear to substantially depress the breathing efforts of babies either at birth or in the first hours of life. It is also reassuring that benefit is seen regardless of the reason for preterm birth and that antenatal magnesium sulphate has similar effects across a range of preterm gestational ages. As there is minimal variation in outcomes related to time to birth and with dosage, it would be prudent to restrict administration of antenatal magnesium sulphate for fetal neuroprotection to close to the expected or planned birth and to use 4 g, the smallest effective dose, with or without a 1 g/hour maintenance dose.
Supporting Information
Zdroje
1. Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet 2012;379(9832):2162–72. doi: 10.1016/S0140-6736(12)60820-4 22682464
2. Chow SSW, Le Marsney R, Hossain S, Haslam R, Lui K. 2015. Report of the Australian and New Zealand Neonatal Network 2013. Sydney.
3. World Health Organization. WHO recommendations on interventions to improve preterm birth outcomes. Geneva: WHO 2015.
4. Saigal S, Doyle LW: An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 2008;371(9608):261–269. doi: 10.1016/S0140-6736(08)60136-1 18207020
5. Blencowe H, Lee AC, Cousens S, Bahalim A, Narwal R, Zhong N, et al. Preterm birth-associated neurodevelopmental impairment estimates at regional and global levels for 2010. Pediatr Res 2013; 74(Suppl 1):17–34.
6. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380(9859):2197–223. doi: 10.1016/S0140-6736(12)61689-4 23245608
7. Kuban KCK, Leviton A, Pagano M, Fenton T, Strassfeld R, Wolff M. Maternal toxemia is associated with reduced incidence of germinal matrix hemorrhage in premature babies. J Child Neurol 1992;7(1):70–6. doi: 10.1177/088307389200700113 1552156
8. Nelson KB, Grether JK. Can magnesium sulfate reduce the risk of cerebral palsy in very low birthweight infants? Pediatrics 1995;95(2):263–9. 7838646
9. Crowther CA, Hiller JE, Doyle LW, Haslam RR. Effect of magnesium sulfate given for neuroprotection before preterm birth: a randomized controlled trial. JAMA 2003;290(20):2669–76. doi: 10.1001/jama.290.20.2669 14645308
10. Marret S, Marpeau L, Zupan-Simunek V, Eurin D, Lévêque C, Hellot MF, et al. PREMAG trial group Magnesium sulphate given before very-preterm birth to protect infant brain: the randomized controlled PREMAG trial. BJOG. 2007;114 : 310–8.
11. Mittendorf R, Dambrosia J, Pryde PG, Lee KS, Gianopoulos JG, Besinger RE, et al. Association between the use of antenatal magnesium sulfate in preterm labor and adverse health outcomes in infants. Am J Obstet Gynecol 2002;186(6):1111–8. 12066082
12. Altman D, Carroli G, Duley L, Farrell B, Moodley J, Neilson J, et al. Do women with pre-eclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: a randomised placebo-controlled trial. Lancet 2002;359(9321):1877–90. 12057549
13. Rouse DJ, Hirtz DG, Thom E, Varner MW, Spong CY, Mercer BM, et al. A randomized, controlled trial of magnesium sulfate for the prevention of cerebral palsy. N Engl J Med 2008;359(9):895–905. doi: 10.1056/NEJMoa0801187 18753646
14. Doyle LW, Crowther CA, Middleton P, Marret S, Rouse D. Magnesium sulphate for women at risk of preterm birth for neuroprotection of the fetus. Cochrane Database Syst Rev 2009;1:CD004661.
15. The Antenatal Magnesium Sulphate for Neuroprotection Guideline Development Panel. Antenatal Magnesium Sulphate Prior to Preterm Birth for Neuroprotection of the Fetus, Infant and Child: National Clinical Practice Guidelines. Adelaide: The University of Adelaide, 2010.
16. Magee L, Sawchuck D, Synnes A, von Dadelszen P. Magnesium Sulphate for Fetal Neuroprotection Consensus Committee. SOGC Clinical Practice Guideline. Magnesium sulphate for fetal neuroprotection. J Obstet Gynaecol Can 2011;33(5):516–29. 21639972
17. Stewart LA, Tierney JF. To IPD or not to IPD? Advantages and disadvantages of systematic reviews using individual patient data. Eval Health Prof 2002,25(1):76–97. doi: 10.1177/0163278702025001006 11868447
18. Higgins J, Green S, (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]: The Cochrane Collaboration; 2011.
19. Tierney JF, Vale C, Riley R, Smith CT, Stewart L, Clarke M, et al. Individual Participant Data (IPD) Meta-analyses of Randomised Controlled Trials: Guidance on Their Use. PLoS Med 2015 : 12(7): e1001855. doi: 10.1371/journal.pmed.1001855 26196287
20. The AMICABLE Group. Antenatal magnesium individual participant data international collaboration: assessing the benefits for babies using the best level of evidence (AMICABLE). Systematic Reviews 2012;1 : 21 doi: 10.1186/2046-4053-1-21 22587882
21. Stewart LA, Clarke M, Rovers M, Riley RD, Simmonds M, Stewart G, et al. Preferred Reporting Items for Systematic Review and Meta-Analyses of individual participant data: the PRISMA-IPD Statement. JAMA;2015 Apr 28;313(16):1657–65. doi: 10.1001/jama.2015.3656 25919529
22. The Editorial Team. Cochrane Pregnancy and Childbirth Group. About The Cochrane Collaboration (Cochrane Review Groups (CRGs)) 2016, Issue 8. Art No.: PREG.
23. Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011; 343 https://doi.org/10.1136/bmj.d5928.
24. Wolf HT, Hegaard HK, Pinborg AB, Huusom LD. Does antenatal administration of magnesium sulphate prevent cerebral palsy and mortality in preterm infants? A study protocol. AIMS Public Health 2015;2 : 727–9.
25. Crowther CA, Middleton PM, Wilkinson D, Ashwood P, Haslam R. Magnesium sulphate at 30 to 34 weeks' gestational age: neuroprotection trial (MAGENTA) - study protocol. BMC Pregnancy Childbirth 2013 Apr 9;13 : 91. doi: 10.1186/1471-2393-13-91 23570677
26. Bain ES, Middleton PF, Crowther CA. Maternal adverse effects of different antenatal magnesium sulphate regimens for improving maternal and infant outcomes: a systematic review. BMC Pregnancy and Childbirth 2013 13 : 195. doi: 10.1186/1471-2393-13-195 24139447
27. Simpson KR, Knox GE: Obstetrical accidents involving intravenous magnesium sulfate: recommendations to promote patient safety. MCN Am J Matern Child Nurs. 2004,29 (3):161–169. 15123972
28. American College of Obstetricians and Gynecologists Committee on Obstetric Practice, Society for Maternal-Fetal Medicine. Committee Opinion No. 455: Magnesium sulfate before anticipated preterm birth for neuroprotection. Obstet Gynecol 2010; 115(3): 669–71. 20177305
29. Peebles DM, Kenyon AP. Magnesium sulphate to prevent cerebral palsy following preterm birth. RCOG Scientific Impact Paper No. 29 August 2011.
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2017 Číslo 10
- Alternativní léčebné možnosti u hypercholesterolemie při intoleranci statinů
- Vliv kombinace nutraceutik na remodelaci levé komory srdeční u osob s metabolickým syndromem
- Nutraceutika a jejich ovlivnění mírného kardiometabolického rizika
- Princip účinku medu v léčbě chronických i infikovaných ran
- Superoxidovaný roztok a jeho využití v léčbě ran
Nejčtenější v tomto čísle
- Assessing the neuroprotective benefits for babies of antenatal magnesium sulphate: An individual participant data meta-analysis
- Gabapentin, opioids, and the risk of opioid-related death: A population-based nested case–control study
- A combination of plasma phospholipid fatty acids and its association with incidence of type 2 diabetes: The EPIC-InterAct case-cohort study
- Quantifying underreporting of law-enforcement-related deaths in United States vital statistics and news-media-based data sources: A capture–recapture analysis