
The Prevalence of Mental Disorders among the Homeless in Western Countries: Systematic Review and Meta-Regression Analysis
Background:
There are well over a million homeless people in Western Europe and North America, but reliable estimates of the prevalence of major mental disorders among this population are lacking. We undertook a systematic review of surveys of such disorders in homeless people.
Methods and Findings:
We searched for surveys of the prevalence of psychotic illness, major depression, alcohol and drug dependence, and personality disorder that were based on interviews of samples of unselected homeless people. We searched bibliographic indexes, scanned reference lists, and corresponded with authors. We explored potential sources of any observed heterogeneity in the estimates by meta-regression analysis, including geographical region, sample size, and diagnostic method. Twenty-nine eligible surveys provided estimates obtained from 5,684 homeless individuals from seven countries. Substantial heterogeneity was observed in prevalence estimates for mental disorders among the studies (all Cochran's χ2 significant at p < 0.001 and all I2 > 85%). The most common mental disorders were alcohol dependence, which ranged from 8.1% to 58.5%, and drug dependence, which ranged from 4.5% to 54.2%. For psychotic illness, the prevalence ranged from 2.8% to 42.3%, with similar findings for major depression. The prevalence of alcohol dependence was found to have increased over recent decades.
Conclusions:
Homeless people in Western countries are substantially more likely to have alcohol and drug dependence than the age-matched general population in those countries, and the prevalences of psychotic illnesses and personality disorders are higher. Models of psychiatric and social care that can best meet these mental health needs requires further investigation.
Published in the journal:
. PLoS Med 5(12): e225. doi:10.1371/journal.pmed.0050225
Category:
Research Article
doi:
https://doi.org/10.1371/journal.pmed.0050225
Summary
Background:
There are well over a million homeless people in Western Europe and North America, but reliable estimates of the prevalence of major mental disorders among this population are lacking. We undertook a systematic review of surveys of such disorders in homeless people.
Methods and Findings:
We searched for surveys of the prevalence of psychotic illness, major depression, alcohol and drug dependence, and personality disorder that were based on interviews of samples of unselected homeless people. We searched bibliographic indexes, scanned reference lists, and corresponded with authors. We explored potential sources of any observed heterogeneity in the estimates by meta-regression analysis, including geographical region, sample size, and diagnostic method. Twenty-nine eligible surveys provided estimates obtained from 5,684 homeless individuals from seven countries. Substantial heterogeneity was observed in prevalence estimates for mental disorders among the studies (all Cochran's χ2 significant at p < 0.001 and all I2 > 85%). The most common mental disorders were alcohol dependence, which ranged from 8.1% to 58.5%, and drug dependence, which ranged from 4.5% to 54.2%. For psychotic illness, the prevalence ranged from 2.8% to 42.3%, with similar findings for major depression. The prevalence of alcohol dependence was found to have increased over recent decades.
Conclusions:
Homeless people in Western countries are substantially more likely to have alcohol and drug dependence than the age-matched general population in those countries, and the prevalences of psychotic illnesses and personality disorders are higher. Models of psychiatric and social care that can best meet these mental health needs requires further investigation.
Introduction
Around 380,000 individuals in the United Kingdom [1] and 740,000 individuals in the United States [2] are reported to be homeless at any given time. Although most live in sheltered accommodation such as emergency hostels, bed and breakfasts, squats, or other temporary accommodation, a recent US report has estimated that 44% are unsheltered, equivalent to over 300,000 people living on the streets [2].
Many studies have reported high prevalences of various health problems among the homeless. Serious physical morbidity, such as tuberculosis and HIV [3], contributes to an increased age-standardised mortality rate of three to four times that in the general population [4,5]. In addition, a number of surveys have found higher rates of serious mental disorders in homeless individuals, but these investigations show at least 10-fold variations in prevalence. Diagnoses of psychosis range from 2% [6] to 31% [7], depression from 4% [8] to 41% [9], and personality disorder from 3% [9] to 71% [10]. It is has been argued that sample selection, case definition, and diagnostic criteria contribute to this heterogeneity [11], although this hypothesis does not appear to have been formally tested. Furthermore, the closure of large psychiatric institutions [12], the shortage of low-cost housing [13], and a lack of community-based supports and services [14] over the past few decades is thought to have contributed to increasing homelessness among people with mental illness, with resulting increased levels of psychiatric morbidity amongst homeless people [8,15]. With the continued reduction in the numbers of inpatient psychiatric beds, the number and proportion of mentally disordered homeless persons is anticipated to increase further [16,17].
Apart from contributing to increased rates of mortality, including from suicide [5,18] and drug abuse [4], the presence of serious mental disorders in the homeless is likely to contribute to increased rates of violent victimization [19], criminality [20–22], and longer periods of homelessness [23]. The provision of good mental health care would therefore reduce psychiatric morbidity and have other public health benefits.
More reliable estimates of the prevalence of serious mental disorders in the homeless should help inform public policy and development of psychiatric services, particularly in urban centres. The most recent review of homeless and mental disorders from 2001 was descriptive and did not attempt a quantitative synthesis of the evidence, or explore the heterogeneity between studies [3]. We report a systematic review and meta-regression analysis of psychiatric surveys of homeless populations in Western countries.
Methods
We searched for surveys that estimated the prevalence of psychotic illness, major depression, personality disorder, alcohol dependence, and substance dependence in homeless people, published between January 1966 and December 2007. We searched computer-based literature indexes (EMBASE, MEDLINE, PsycINFO), scanned relevant reference lists, searched relevant journals by hand, and corresponded with authors. For the database search, we used combinations of keywords relating to psychiatric illnesses (e.g., mental*, psych*, depress*, substance/drug*/alcohol* abuse/dependence, personality) and being homeless (e.g., homeless*, roofless, shelter*). Non-English articles were translated. MOOSE guidelines were followed (Text S1).
For inclusion into the systematic review, the studies had to meet the following criteria: (1) A clear definition of homelessness was included; (2) standardized diagnostic criteria for psychiatric disorders using the International Classification of Diseases: Classification of Mental and Behavioural Disorders (ICD) or Diagnostic and Statistical Manual of Mental Disorders (DSM) were used; (3) psychiatric diagnosis was made by clinical examination or interviews using validated diagnostic instruments; (4) prevalence rates for psychiatric disorders within the previous six months were included, except for personality disorder where lifetime diagnoses were used; (5) study location was in North America, Western Europe, Australia, and New Zealand.
Surveys with less than a 50% response rate were excluded, as were surveys on selected populations (for example, a sample of homeless people referred to a psychiatric outpatient clinic or single mothers [24]) or where diagnosis of psychiatric disorders was not obtained by direct interviews (for example, by self report or case note review) or was only reported as 12-mo or lifetime diagnoses [16,25–29]. Studies that selected solely elderly or juvenile people were excluded [30,31]. All the included reports were based on interviews with individuals. We identified one study that interviewed families, but this was excluded as it was based on a selected sample [32].
Information on geographical location; year of interview; definition of homelessness; method of sample selection; sample size; average age; diagnostic instrument; diagnostic criteria, type of interviewer, participation rate; and numbers diagnosed with psychotic illness, major depression, personality disorder, alcohol dependence, and drug dependence was extracted independently from every eligible study. If required, further clarifications were sought by correspondence with authors of relevant studies.
Prevalence estimates were calculated using the variance stabilising double arcsine transformation [33], because of the use of the inverse variance weight in fixed-effects meta-analysis is suboptimal when dealing with binary data with low prevalences. In addition, the transformed prevalences are weighted very slightly towards 50% and studies with zero prevalence can thus be included in the analysis. Confidence intervals (CIs) around these estimates were calculated using the Wilson method [34] since the asymptotic method produces intervals which can extend below zero [35]. Heterogeneity among studies was estimated using Cochran's Q (reported with a χ2-value and p-value) and the I2 statistic, the latter describing the percentage of variation across studies that is due to heterogeneity rather than chance [36,37], and presented with a 95% CI [37]. I2, unlike Q, does not inherently depend upon the number of studies considered, with values of 25%, 50%, and 75% taken to indicate low, moderate, and high levels of heterogeneity, respectively. Where heterogeneity was high (I2 > 75%), random effects models were used for summary statistics [36]. In situations with high between-study heterogeneity, the use of random effects models (where the individual study weight is the sum of the weight used in a fixed effects model and the between-study variability) produces study weights that primarily reflect the between-study variation and thus provide close to equal weighting. The use of the arcsine-transformed prevalence estimates consequently had little material difference on the value of the overall random effects estimates, which were themselves found to be notably different (closer to 50%) from the fixed effects estimates in which smaller prevalences have smaller standard errors and thus greater weight. Potential sources of heterogeneity were investigated further by arranging groups of studies according to potentially relevant characteristics and by meta-regression analysis. Factors examined both individually and in multiple variable models were instrument (semistructured instrument versus clinical examination only), interviewer (conducted by mental health clinician or not), period (decade of study: 1970s, 1980s, 1990s, and 2000s), study size (both a continuous variable and as a categorical variable in increments of n = 50 and n = 100, and also as n < 200 versus n ≥ 200), sex (as appropriate, e.g., male versus female; mixed versus male versus female), geographical region (as appropriate, e.g., mainland Europe versus rest of Western countries), and participation rates (classified into those >85% and those ≤85%). Because of low prevalence and small sample size for some studies, only those factors significant (p < 0.10) individually were entered into a multiple regression model to avoid model instability. The regression coefficients for each study characteristic on individual analysis were provided to enable comparison across diagnoses. All analyses were done in STATA statistical software package, version 10 (Statacorp, 2007) using the commands propcii (to calculate Wilson CIs), metan (for random effects meta-analysis, specifying either two or three variables: double arcsine transformed prevalence and its variance, or double arcsine transformed prevalence and Wilson CIs), and metareg (for meta-regression).
Results
The final sample consisted of 29 studies published between 1979 and 2005 (Table 1) [6–10,38–59]. The studies included a total of 5,684 homeless individuals. Eleven reports reported data on men (n = 1,827) [7,38,40–43,45,47–49,60], 14 included mixed gender samples (n = 3,381) [6,8,39,44,50–54,61], and four investigated women (n = 476) [9,10,40,55]. In the surveys with mixed samples, 82% of the individuals were men (weighted average). The weighted average age of men (reported in eight reports) and women (from four reports) was 41.2 and 33.8 y, respectively. Average age of the mixed samples was 40.1 y (from ten studies). Ten studies were published before 1990 [6–8,10,39,40,42,45,46,49]. Ten reports were from the US (n = 2,019) [6,8,10,38,39,42,49,51,52,55], eight from the UK (n = 1645) [7,44,45,53,56–58,61], six from Germany (n = 624) [9,41,47,48,59,60], two from Australia (n = 473) [40,46], and one each from France (n = 715) [50], The Netherlands (n = 150) [43], and Greece (n = 58) [54].

Different sampling strategies (random methods, consecutive sampling or total sampling) were used in surveys, apart from two reports that did not provide information on sampling method [59,60]. Of the 5,684 homeless individuals, 952 were selected primarily from shelters for the homeless, 583 from hostels for the homeless, and the rest from a mixture of settings including day centres, soup kitchens, missions, streets, and shelters. Eight studies reported response rate of above 90% [6–8,38,45,49,53,55], the others were mostly above 70%. Three reports did not provide response rates [54,56,61], a further one did not cite the response rate for part of the sample [40], and five surveys reported response rates between 60% and 70% [42–44,47,52].
In six surveys, diagnosis of psychotic illness, major depression, personality disorder, alcohol dependence, and drug dependence was made by clinical examination without the use of diagnostic instruments (n = 600) [7,8,10,51,54]. Validated semistructured diagnostic instruments used included: Diagnostic Interview Schedule (DIS) (n = 1,455) [6,9,38,39,52,55]; Clinical Interview Schedule, Revised (CIS-R) (n = 1,090) [57,58]; Structured Clinical Interview for Diagnostic and Statistical Manual (SCID) (n = 1,081) [40,41,47,56,59]; Present State Examination (PSE) (n = 394) [44,45,49,53], and the Composite International Diagnostic Interview (CIDI) (n = 724) [43,48,50]. Three other studies used clinical semistructured interviews [48,60,61].
Psychotic Illness
Psychotic illness was reported in 28 surveys with a random effects pooled prevalence of 12.7% (95% CI 10.2%–15.2%) [6–10,38–56,60,61]. Estimates ranged from 2.8% to 42.3% with substantial heterogeneity among the estimates (χ2 = 237.7, p < 0.001, I2 = 88.6%, 95% CI 84.8%–91.5%). Higher prevalences were found in smaller studies (Figure 1). We further explored study region, grouping studies according to whether they were based in mainland Europe, UK, US, or Australasia (Figure 2). In individual variable meta-regression analyses, surveys in which the interviewer was a mental health clinician (versus a lay interviewer) had higher prevalences of psychosis (β = 0.08, standard error [se(β)] = 0.04, p = 0.042), where the participation rates were lower (<85%) had lower prevalences (β = −0.06, se[β] = 0.03, p = 0.071) (Figure 3), and where the study size was 200 or more participants (versus fewer than 200) had lower prevalences (β = −0.08, se[β] = 0.04, p = 0.055) (Table 2). In a meta-regression model including these three characteristics, only the participation rate remained significant: lower participation rates were associated with lower prevalences (β = −0.08, se[β] = 0.03, p = 0.015).




Major Depression
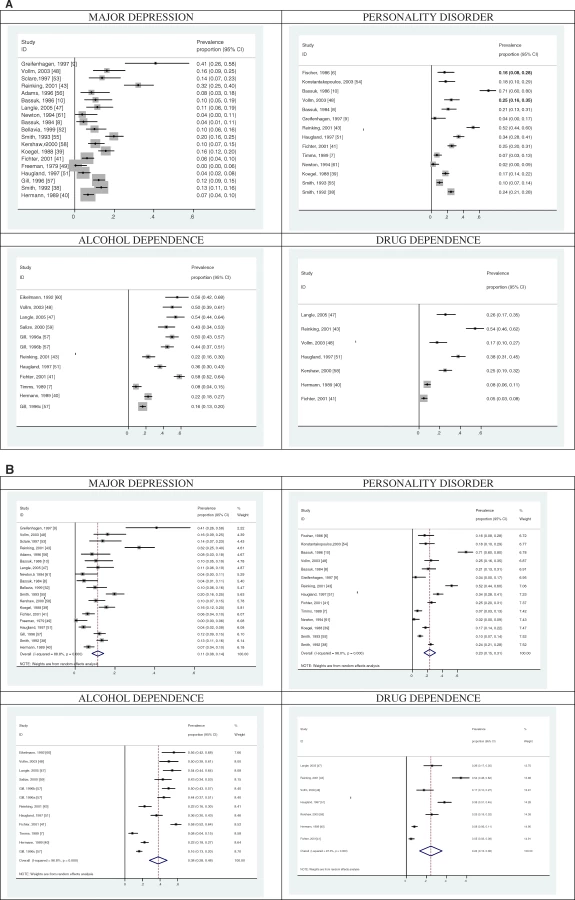
We identified 19 surveys that reported major depression with a random effects pooled prevalence estimate of 11.4% (95% CI 8.4%–14.4%) (Figure 4) [8–10,38–41,43,47–49,51–53,55–58,61]. The prevalence estimates ranged from 0.0% to 40.9% and there was substantial heterogeneity among those estimates (χ2 = 160.6, p < 0.001, I2 = 88.8%, 95% CI 84.0%–92.2%). Four factors were associated with this heterogeneity on meta-regression: the interview being conducted by a mental health clinician, where there were lower prevalences (β = −0.06, se[β] = 0.04, p = 0.058); the study being conducted in mainland Europe compared with the rest of the world (β = −0.09, se[β] = 0.04, p = 0.024); sex (coded as female, male, mixed), with men and mixed samples having progressively lower prevalences than women (β = −0.05, se[β] = 0.02, p = 0.043); and participation rate, with lower participation rates being associated with higher prevalences (β = 0.13, se[β] = 0.03, p < 0.001) (Table 2). In a meta-regression model including these four characteristics, only the participation rate remained significant: lower participation rates were associated with higher prevalences (β = 0.11, se[β] = 0.03, p = 0.002).
Personality Disorder
We identified 14 surveys that reported personality disorder diagnoses in 2,413 homeless persons (Figure 4) [6–10,38,39,41,48,51,54,55,61]. The prevalence estimates ranged from 2.2% to 71.0%. The random effects pooled prevalence estimate was 23.1% (95% CI 15.5%–30.8%) (χ2 = 327.5, p < 0.001, I2 = 96.0%, 95% CI 94.6%–97.1%), with only one of the sample characteristics being significantly associated with this substantial heterogeneity on individual variable analysis: lower participation rates were associated with higher prevalences (β = 0.29, se[β] = 0.08, p < 0.001) (Table 2).
Alcohol Dependence
We identified ten surveys that reported alcohol dependence in 1,791 homeless men (Figure 4) [7,40,41,43,47,48,51,57,59,60]. The prevalence estimates ranged from 8.5% to 58.1%. The random effects pooled prevalence estimate was 37.9% (95% CI 27.8%–48.0%) (χ2 = 347.2, p < 0.001, I2 = 96.8%, 95% CI 95.7%–97.7%). Two factors were associated with this heterogeneity on individual but not multiple variable analysis. First, the more recent the study (as analysed by decade), the higher the prevalence of alcohol dependence (β = 0.18, se[β] = 0.07, p = 0.007, Figure 5). Second, surveys conducted in mainland Europe had higher prevalences of alcohol dependence (β = 0.21, se[β] = 0.09, p = 0.022) (Table 2). We did not find any investigations of alcohol dependence in homeless women.

Drug Dependence
We identified seven surveys in men that reported drug dependence (Figure 4) [40,41,43,47,48,51,58]. The prevalence estimates ranged from 4.7% to 54.2%. Random effects pooled prevalence estimate was 24.4% (95% CI 13.2%–35.6%) (χ2 = 221.1, p < 0.001, I2 = 97.3%, 95% CI 95.9%–98.2%), with none of the sample characteristics being significantly associated with this heterogeneity on individual variable analysis (Table 2). We found one report on drug dependence in homeless women (n = 33) with a prevalence of 24.2% [58].
Conclusion
This systematic review of serious mental disorders in homeless persons identified 29 surveys including 5,684 individuals. There are three main findings. First, the most common mental disorders appeared to be alcohol and drug dependence, with random effects pooled prevalence estimates of 37.9% (95% CI 27.8%–48.0%) and 24.4% (95% CI 13.2%–35.6%), respectively. Second, the prevalence estimates for psychosis were at least as high as those for depression, a finding in marked contrast from community estimates of these conditions [62,63], and in other at-risk groups such as prisoners [64] and refugees [65], in whom depression is more common. Third, although high prevalences were reported for serious mental disorders, their substantial heterogeneity suggests that service planning should not rely on our summary estimates but commission local surveys of morbidity to quantify mental health needs.
The substantial heterogeneity between the studies included in the review was not unexpected. Some of the variations between studies could be not explained by crude study characteristics (such as sex, study size, or geographic region), and this suggests that local factors such as provision of mental health and social services are likely to be important [66]. However, certain other study characteristics were associated with heterogeneity on meta-regression. These included, first, lower participation in surveys were associated with lower prevalences of psychosis. Second, interviewers with clinical training were more likely to reporting lower prevalences of depression. Third, a higher prevalence of alcohol dependence was found in studies in more recent decades, possibly reflecting the increasing relative affordability of alcohol [67,68].
The prevalence of psychosis ranged between 3% and 42%, which is substantially higher than community estimates, which typically report 1%–2% when individuals are surveyed using diagnostic instruments [69], and up to 0.8% when only schizophrenia is reported [70]. We found no increase in the prevalence of psychosis by study period (in decades), in contrast with the views of some commentators [15,16]. The finding on meta-regression that the proportion of the individuals who participated was significantly associated with these prevalences suggests that researchers in the field need to interpret their findings in light of response rates. Reasons for nonparticipation in research may be related to severe mental illness, and investigators should consider gathering information from other sources to estimate the degree of underestimation or attempt to reinterview those who did not participate initially.
Although the proportionate excess for psychosis was greater than for the other mental disorders, this review found that the main mental health problem for homeless persons is alcohol dependence, which ranged from 8% to 58%. On average, this is many orders of magnitude higher in men and even higher in women compared with community surveys [62,63]. The range for drug dependence were 5%–54%, a proportionate excess higher in women than men compared with community surveys [62,63]. The increased prevalence for drug dependence in both sexes may contribute to the reported increased crime rates in the homeless [20,21,22], as substance abuse and dependence is an important risk factor, either alone [71] or comorbid with psychosis [21].
The prevalence of depression in this review, with a pooled prevalence estimate of 11.4% (95% CI 8.4%–14.4%), range at 0% to 41%, was lower than expected. Many estimates included in the review were similar to community estimates of depression in women (which range from 7% to 11% for 1-y estimates), and only slightly higher than general population rates for men [62,72]. While levels of comorbidity of depression are likely to be underreported in homeless persons with psychosis or drug dependence, these estimates suggest that the reported high rates of suicide in homeless people [5,18] may not be mediated through depressive illness, and that other risk factors, such alcohol dependence, may be more relevant [73]. The finding that clinically trained interviewers were associated with lower prevalence estimates is consistent with a systematic review of major depressive disorder in prisoners [64], and suggests that studies of the diagnostic validity of depression using different types of interviewer should be researched. In terms of the prevalence of personality disorder in the homeless, we found that the estimates varied widely (range 2.2%–71.0%), and all but one reported rates higher than the 4.4% found in a recent community survey [74]. The presence of personality disorder is associated with poorer outcomes for treatment of depression [75] and increased risk of deliberate self-harm [76].
One of the findings of this review is that future research in homeless populations should provide clear definitions of the sample interviewed and breakdowns by type of homelessness category (whether it be roofless or temporary accommodation). Although we identified and excluded from the review one study from a non-Western population (South Korea) [77], it highlighted the need for research in non-Western countries. Longitudinal studies of cohorts of the mentally ill would help clarify the risk for, temporal sequence of, and pathways into homelessness, and identify risk factors and those associated with desistence for homelessness in such populations.
A number of implications for health services for the homeless arise from this review. Integrating treatment for mental illness, substance dependence, and housing interventions should be considered for many homeless persons [78,79], and hospital admission may be required for treatment for a number with psychotic illness. Local surveys are needed to inform service needs. However, traditional models of service delivery in Western countries, which focus on those with severe mental illness, may not meet the mental health needs of most homeless people who suffer from substance dependence and personality disorder. Even when mentally ill homeless persons receive adequate mental health services, a range of unmet welfare and housing needs may remain, implying that normal community mental health service provision is usually insufficient [80]. With many millions of individuals being homeless in Western countries, current mental health provision may need review, and models of psychiatric and social care that can best meet the burden of mental illness will need further investigation.
Supporting Information
Zdroje
1. Crisis
2003
How many and how much: Single homelessness and the question of numbers and cost
London
Crisis UK
2. Homelessness Research Institute
2007
Homelessness counts
Washington (D.C)
National Alliance to End Homelessness
3. MartensW
2001
A review of physical and mental health in homeless persons.
Public Health Rev
29
13
33
4. BarrowSMHermanDBCordovaPStrueningEL
1999
Mortality among homeless shelter residents in New York City.
Am J Public Health
89
529
534
5. BabidgeNCBuhrichNButlerT
2001
Mortality among homeless people with schizophrenia in Sydney, Australia: A ten year follow-up.
Acta Psychiatr Scand
103
105
110
6. FischerPJShapiroSBreakeyWRAnthonyJCKramerM
1986
Mental health and social characteristics of the homeless: A survey of mission users.
Am J Public Health
76
519
524
7. TimmsPWFryAH
1989
Homelessness and mental illness.
Health Trends
21
70
71
8. BassukELRubinLLauriatA
1984
Is homelessness a mental health problem.
Am J Psychiatry
141
1546
1550
9. GreifenhagenAFichterM
1997
Mental illness in homeless women: An epidemiological study in Munich, Germany.
Eur Arch Psychiatry Clin Neurosci
247
162
172
10. BassukELRubinLLauriatAS
1986
Characteristics of sheltered homeless families.
Am J Public Health
76
1097
1101
11. FischerPJ
1989
Estimating the prevalence of alcohol, drug and mental health problems in the contemporary homeless population: a review of the literature.
Contemp Drug Probl
16
333
390
12. ApplebyLDesaiPN
1985
Documenting the relationship between homelessness and psychiatric hospitalization.
Hosp Comm Psychiatry
37
732
737
13. WrightJLamJ
1987
Homelessness and the low-income housing supply.
Soc Policy
17
48
53
14. KushelMVittinghoffEHaasJ
2001
Factors associated with the health care utilization of homeless persons.
JAMA
285
200
206
15. LambHR
1984
Deinstitutionalisation and the homeless mentally ill.
Hosp Comm Psychiatry
35
899
907
16. NorthCSEyrichKMPollioDESpitznagelEL
2004
Are rates of psychiatric disorders in the homeless population changing.
Am J Public Health
94
103
108
17. TeesonM
1990
Prevalence of schizophrenia in a refuge for homeless men: A five year follow-up.
Psychiatric Bull
14
597
600
18. PrigersonHGDesaiRALiu-MaresWRosenheckRA
2003
Suicidal ideation and suicide attempts in homeless mentally ill persons: Age-specific risks of substance abuse.
Soc Psychiatry Psychiatr Epidemiol
38
213
219
19. WalshEMoranPScottCMcKenzieKBurnsT
2003
Prevalence of violent victimisation in severe mental illness.
Br J Psychiatry
183
233
238
20. GelbergLLinnLSLeakeBD
1988
Mental health, alcohol and drug use, and criminal history among homeless adults.
Am J Psychiatry
145
191
196
21. BrennanPMednickSHodginsS
2000
Major mental disorders and criminal violence in a Danish birth cohort.
Arch Gen Psychiatry
57
494
500
22. FazelSGrannM
2006
The population impact of severe mental illness on violent crime.
Am J Psychiatry
163
1397
1403
23. MorseGShieldsNMHannekeCRMcCallGJCalsynRJ
1986
St. Louis's homeless: Mental health needs, services, and policy implications.
Psychosocial Rehab J
9
39
50
24. BassukELBucknerJCPerloffJNBassukSS
1998
Prevalence of mental health and substance use disorders among homeless and low-income housed mothers.
Am J Psychiatry
155
1561
1564
25. TeessonSHodderTBuhrichN
2000
Substance use disorders among homeless people in inner Sydney.
Soc Psychiat Psychiatr Epidemiol
35
451
456
26. TeessonMHodderTBuhrichN
2004
Psychiatric disorders in homeless men and women in inner Sydney.
Aust N Z J Psychiatry
38
162
168
27. VirgonaABuhrichNTeessonM
1993
Prevalence of schizophrenia among women in refuges for the homeless.
Aust N Z J Psychiatry
27
405
410
28. VazquezCMunozMSanzJ
1997
Lifetime and 12-month prevalence of DSM-III-R mental disorders among the homeless in Madrid: A European study using the CIDI.
Acta Psychiatr Scand
95
523
530
29. LovisiGMannACoutinhoEMorgadoA
2004
Mental illness in an adult sample admitted to public hostels in the Rio de Janeiro metropolitan area, Brazil.
Soc Psychiat Psychiatr Epidemiol
38
493
498
30. PriestRG
1976
The homeless person and the psychiatric services: an Edinburgh survey.
Br J Psychiatry
128
128
136
31. ReillyJJHerrmanHEClarkeDMNeilCCMcNamaraCL
1994
Psychiatric disorder in and service use by young homeless people.
Med J Aust
161
429
432
32. VostanisPGrattanECumellaS
1998
Mental health problems of homeless children and families: longitudinal study.
BMJ
316
899
902
33. FreemanMTukeyJ
1950
Transformations related to the angular and the square root.
Ann Math Stats
4
607
611
34. WilsonE
1927
Probable inference, the law of succession, and statistical inference.
J Am Stat Assoc
22
209
212
35. NewcombeR
1998
Two-sided confidence intervals for the single proportion: comparison of seven methods.
Stats Med
17
857
872
36. HigginsJThompsonSDeeksJAltmanD
2003
Measuring inconsistency in meta-analyses.
BMJ
327
557
560
37. HigginsJThompsonS
2002
Quantifying heterogeneity in a meta-analysis.
Stats Med
21
1539
1558
38. SmithEMNorthCSSpitznagelEL
1992
A systematic study of mental illness, substance abuse, and treatment in 600 homeless men.
Ann Clin Psychiatry
4
111
120
39. KoegelPBurnamMAFarrRK
1988
The prevalence of specific psychiatric disorders among homeless individuals in the inner city of Los Angeles.
Arch Gen Psychiatry
45
1085
1092
40. HerrmanHMcGorryPBennettPVan RielRSinghB
1989
Prevalence of severe mental disorders in disaffiliated and homeless people in inner Melbourne.
Am J Psychiatry
146
1179
1184
41. FichterMMQuadfliegN
2001
Prevalence of mental illness in homeless men in Munich, Germany: Results from a representative sample.
Acta Psychiatr Scand
103
94
104
42. SusserEStrueningELConoverS
1989
Psychiatric problems in homeless men. Lifetime psychosis, substance use, and current distress in new arrivals at New York City shelters.
Arch Gen Psychiatry
46
845
850
43. ReinkingDPWolfJRKroonH
2001
Hoge prevalentie van psychische stoornissen en verslavingsproblemen bij daklozen in de stad Utrecht [High prevalence of mental disorders and addiction problems among the homeless in Utrecht].
Ned Tijdschr Geneeskd
145
1161
1166
44. GeddesJNewtonRYoungGBaileySFreemanC
1994
Comparison of prevalence of schizophrenia among residents of hostels for homeless people in 1966 and 1992.
BMJ
308
816
819
45. WellerBGWellerMPCokerEMahomedS
1987
Crisis at Christmas 1986.
Lancet
1
553
554
46. DoutneyCPBuhrichNVirgonaACohenADanielsP
1985
The prevalence of schizophrenia in a refuge for homeless men.
Aust N Z J Psychiatry
19
233
238
47. LangleGEgerterBAlbrechtFPetraschMBuchkremerG
2005
Prevalence of mental illness among homeless men in the community - Approach to a full census in a southern German university town.
Soc Psychiatry Psychiatr Epidemiol
40
382
390
48. VollmBBeckerHKunstmannW
2004
Psychiatrische Morbidität bei allein stehenden wohnungslosen Männern [Psychiatric morbidity in homeless single men].
Psychiatr Prax
31
236
240
49. FreemanSJFormoAAlampurAGSommersAF
1979
Psychiatric disorder in a skid-row mission population.
Compr Psychiatry
20
454
462
50. KovessVMangin LazarusC
1999
The prevalence of psychiatric disorders and use of care by homeless people in Paris.
Soc Psychiatry Psychiatr Epidemiol
34
580
587
51. HauglandGSiegelCHopperKAlexanderMJ
1997
Mental illness among homeless individuals in a suburban county.
Psychiatr Serv
48
504
509
52. BellaviaCWToroPA
1999
Mental disorder among homeless and poor people: a comparison of assessment methods.
Community Ment Health J
35
57
67
53. SclarePD
1997
Psychiatric disorder among the homeless in Aberdeen.
Scot Med J
42
173
177
54. KonstantakopoulosGKakoulasIValmaVStamatogiannopoulouEGiotakosO
2003
Mental disorders and dual diagnosis in a sample of homeless people in Athens.
Annals Gen Hosp Psychiatry
2
Suppl 1
S113
55. SmithEMNorthCSSpitznagelEL
1993
Alcohol, drugs, and psychiatric comorbidity among homeless women: an epidemiologic study.
J Clin Psychiatry
54
82
87
56. AdamsCEPantelisCDukePJBarnesTR
1996
Psychopathology, social and cognitive functioning in a hostel for homeless women.
Br J Psychiatry
168
82
86
57. GillBMeltzerHHindsKPetticrewM
1996
Psychiatric morbidity among homeless people
London
HMSO
58. KershawASingletonNMeltzerH
2000
Substance misuse and mental disorder among homeless people in Glasgow
London
ONS
59. SalizeHJDillmann-LangeCSternGKentner-FiguraBStammK
2002
Alcoholism and somatic comorbidity among homeless people in Mannheim, Germany.
Addiction
97
1593
1600
60. EikelmannBInhesterMLRekerT
1992
Psychische Störungen bei nicht-sesshaften Männern. Defizite in der psychiatrischen Versorgung.
Sozialpsychiatrische Informationen
2
29
32
61. NewtonJRGeddesJRBaileySFreemanCPMcAleavyA
1994
Mental health problems of the Edinburgh 'roofless'.
Br J Psychiatry
537
540
62. KesslerRMcGonagleKZhaoS
1994
Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States.
Arch Gen Psychiatry
51
8
19
63. KesslerRCChiuWTDemlerOWaltersEE
2005
Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the national comorbidity survey replication.
Arch Gen Psychiatry
62
617
627
64. FazelSDaneshJ
2002
Serious mental disorder in 23 000 prisoners: a systematic review of 62 surveys.
Lancet
359
545
550
65. FazelMWheelerJDaneshJ
2005
Prevalence of serious mental disorder in 7000 refugees resettled in western countries: A systematic review.
Lancet
365
1309
1314
66. TischlerVCumellaSBellerbyTVostanisP
2000
Service innovations: A mental health service for homeless children and families.
Psychiatr Bull
24
339
341
67. FarrellSManningWGFinchMD
2003
Alcohol dependence and the price of alcoholic beverages.
J Health Econ
22
117
147
68. RoomR
2005
Alcohol and public health.
Lancet
365
519
69. RobinsRReigerD
1991
Psychiatric disorders in America: The Epidemiologic Catchment Area Study
New York
The Free Press
70. SahaSChantDWelhamJMcGrathJ
2005
A systematic review of the prevalence of schizophrenia.
PLoS Medicine
2
e141
doi:10.1371/journal.pmed.0020141
71. GrannMFazelS
2004
Substance misuse and violent crime: Swedish population study.
BMJ
328
1233
1234
72. KesslerRCBerglundPDemlerOJinRKoretzD
2003
The Epidemiology of Major Depressive Disorder: Results From the National Comorbidity Survey Replication (NCS-R).
JAMA
289
3095
3105
73. CavanaghJCarsonASharpeMLawrieS
2003
Psychological autopsy studies of suicide: a systematic review.
Psychol Med
33
395
405
74. CoidJYangMTyrerPRobertsAUllrichS
2006
Prevalence and correlates of personality disorders in Great Britain.
Br J Psychiatry
188
423
431
75. Newton-HowesGTyrerPJohnsonT
2006
Personality disorder and the outcome of depression: meta-analysis of published studies.
Br J Psychiatry
188
13
20
76. HawtonKHoustonKHawCTownsendEHarrissL
2003
Comorbidity of axis I and axis II disorders in patients who attempted suicide.
Am J Psychiatry
160
1494
1500
77. HanOSLeeHBAhnJHParkJIChoMJ
2003
Lifetime and current prevalence of mental disorders among homeless men in Korea.
J Nerv Ment Dis
4
272
275
78. DrakeRYovetichNBeboutRHarrisMMcHugoG
1997
Integrated treatment for dually diagnosed homeless adults.
J Nerv Ment Dis
185
298
305
79. GoldfingerSMSchuttRKTolomiczenkoGSSeidmanLPenkWE
1999
housing placement and subsequent days homeless among formerly homeless adults with mental illness.
Psychiatr Serv
50
674
679
80. HerrmanHEvertHHarveyCGurejeOPinzoneT
2004
Disability and service use among homeless people living with psychotic disorders.
Aust N Z J Psychiatry
38
965
974
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2008 Číslo 12
- Alternativní léčebné možnosti u hypercholesterolemie při intoleranci statinů
- Vliv kombinace nutraceutik na remodelaci levé komory srdeční u osob s metabolickým syndromem
- Nutraceutika a jejich ovlivnění mírného kardiometabolického rizika
- Princip účinku medu v léčbě chronických i infikovaných ran
- Superoxidovaný roztok a jeho využití v léčbě ran
Nejčtenější v tomto čísle
- Homelessness Is Not Just a Housing Problem
- The Dirty War Index: A Public Health and Human Rights Tool for Examining and Monitoring Armed Conflict Outcomes
- Accessing Maternal Health Services in Eastern Burma
- Poverty and Cataract—A Deeper Look at a Complex Issue