
Effects of Hormone Therapy on Cognition and Mood in Recently Postmenopausal Women: Findings from the Randomized, Controlled KEEPS–Cognitive and Affective Study
Background:
Menopausal hormone therapy (MHT) reportedly increases the risk of cognitive decline in women over age 65 y. It is unknown whether similar risks exist for recently postmenopausal women, and whether MHT affects mood in younger women. The ancillary Cognitive and Affective Study (KEEPS-Cog) of the Kronos Early Estrogen Prevention Study (KEEPS) examined the effects of up to 4 y of MHT on cognition and mood in recently postmenopausal women.
Methods and Findings:
KEEPS, a randomized, double-blinded, placebo-controlled clinical trial, was conducted at nine US academic centers. Of the 727 women enrolled in KEEPS, 693 (95.3%) participated in the ancillary KEEPS-Cog, with 220 women randomized to receive 4 y of 0.45 mg/d oral conjugated equine estrogens (o-CEE) plus 200 mg/d micronized progesterone (m-P) for the first 12 d of each month, 211 women randomized to receive 50 μg/d transdermal estradiol (t-E2) plus 200 mg/d m-P for the first 12 d of each month, and 262 women randomized to receive placebo pills and patches. Primary outcomes included the Modified Mini-Mental State examination; four cognitive factors: verbal learning/memory, auditory attention/working memory, visual attention/executive function, and speeded language/mental flexibility; and a mood measure, the Profile of Mood States (POMS). MHT effects were analyzed using linear mixed-effects (LME) models, which make full use of all available data from each participant, including those with missing data. Data from those with and without full data were compared to assess for potential biases resulting from missing observations. For statistically significant results, we calculated effect sizes (ESs) to evaluate the magnitude of changes.
On average, participants were 52.6 y old, and 1.4 y past their last menstrual period. By month 48, 169 (24.4%) and 158 (22.8%) of the 693 women who consented for ancillary KEEPS-Cog were lost to follow-up for cognitive assessment (3MS and cognitive factors) and mood evaluations (POMS), respectively. However, because LME models make full use all available data, including data from women with missing data, 95.5% of participants were included in the final analysis (n = 662 in cognitive analyses, and n = 661 in mood analyses). To be included in analyses, women must have provided baseline data, and data from at least one post-baseline visit. The mean length of follow-up was 2.85 y (standard deviation [SD] = 0.49) for cognitive outcomes and 2.76 (SD = 0.57) for mood outcomes. No treatment-related benefits were found on cognitive outcomes. For mood, model estimates indicated that women treated with o-CEE showed improvements in depression and anxiety symptoms over the 48 mo of treatment, compared to women on placebo. The model estimate for the depression subscale was −5.36 × 10−2 (95% CI, −8.27 × 10−2 to −2.44 × 10−2; ES = 0.49, p < 0.001) and for the anxiety subscale was −3.01 × 10−2 (95% CI, −5.09 × 10−2 to −9.34 × 10−3; ES = 0.26, p < 0.001). Mood outcomes for women randomized to t-E2 were similar to those for women on placebo. Importantly, the KEEPS-Cog results cannot be extrapolated to treatment longer than 4 y.
Conclusions:
The KEEPS-Cog findings suggest that for recently postmenopausal women, MHT did not alter cognition as hypothesized. However, beneficial mood effects with small to medium ESs were noted with 4 y of o-CEE, but not with 4 y of t-E2. The generalizability of these findings is limited to recently postmenopausal women with low cardiovascular risk profiles.
Trial Registration: ClinicalTrials.gov NCT00154180 and NCT00623311
Published in the journal:
. PLoS Med 12(6): e32767. doi:10.1371/journal.pmed.1001833
Category:
Research Article
doi:
https://doi.org/10.1371/journal.pmed.1001833
Summary
Background:
Menopausal hormone therapy (MHT) reportedly increases the risk of cognitive decline in women over age 65 y. It is unknown whether similar risks exist for recently postmenopausal women, and whether MHT affects mood in younger women. The ancillary Cognitive and Affective Study (KEEPS-Cog) of the Kronos Early Estrogen Prevention Study (KEEPS) examined the effects of up to 4 y of MHT on cognition and mood in recently postmenopausal women.
Methods and Findings:
KEEPS, a randomized, double-blinded, placebo-controlled clinical trial, was conducted at nine US academic centers. Of the 727 women enrolled in KEEPS, 693 (95.3%) participated in the ancillary KEEPS-Cog, with 220 women randomized to receive 4 y of 0.45 mg/d oral conjugated equine estrogens (o-CEE) plus 200 mg/d micronized progesterone (m-P) for the first 12 d of each month, 211 women randomized to receive 50 μg/d transdermal estradiol (t-E2) plus 200 mg/d m-P for the first 12 d of each month, and 262 women randomized to receive placebo pills and patches. Primary outcomes included the Modified Mini-Mental State examination; four cognitive factors: verbal learning/memory, auditory attention/working memory, visual attention/executive function, and speeded language/mental flexibility; and a mood measure, the Profile of Mood States (POMS). MHT effects were analyzed using linear mixed-effects (LME) models, which make full use of all available data from each participant, including those with missing data. Data from those with and without full data were compared to assess for potential biases resulting from missing observations. For statistically significant results, we calculated effect sizes (ESs) to evaluate the magnitude of changes.
On average, participants were 52.6 y old, and 1.4 y past their last menstrual period. By month 48, 169 (24.4%) and 158 (22.8%) of the 693 women who consented for ancillary KEEPS-Cog were lost to follow-up for cognitive assessment (3MS and cognitive factors) and mood evaluations (POMS), respectively. However, because LME models make full use all available data, including data from women with missing data, 95.5% of participants were included in the final analysis (n = 662 in cognitive analyses, and n = 661 in mood analyses). To be included in analyses, women must have provided baseline data, and data from at least one post-baseline visit. The mean length of follow-up was 2.85 y (standard deviation [SD] = 0.49) for cognitive outcomes and 2.76 (SD = 0.57) for mood outcomes. No treatment-related benefits were found on cognitive outcomes. For mood, model estimates indicated that women treated with o-CEE showed improvements in depression and anxiety symptoms over the 48 mo of treatment, compared to women on placebo. The model estimate for the depression subscale was −5.36 × 10−2 (95% CI, −8.27 × 10−2 to −2.44 × 10−2; ES = 0.49, p < 0.001) and for the anxiety subscale was −3.01 × 10−2 (95% CI, −5.09 × 10−2 to −9.34 × 10−3; ES = 0.26, p < 0.001). Mood outcomes for women randomized to t-E2 were similar to those for women on placebo. Importantly, the KEEPS-Cog results cannot be extrapolated to treatment longer than 4 y.
Conclusions:
The KEEPS-Cog findings suggest that for recently postmenopausal women, MHT did not alter cognition as hypothesized. However, beneficial mood effects with small to medium ESs were noted with 4 y of o-CEE, but not with 4 y of t-E2. The generalizability of these findings is limited to recently postmenopausal women with low cardiovascular risk profiles.
Trial Registration: ClinicalTrials.gov NCT00154180 and NCT00623311
Introduction
Previously referred to as hormone replacement therapy (HRT), supplementation with estrogen and progesterone is prescribed during or after the menopausal transition for management of menopausal symptoms. There is emerging evidence that the cognitive and mood effects of menopausal hormone therapy (MHT) may vary depending on the timing of administration relative to menopause [1,2]. Specifically, it is hypothesized that MHT could potentially enhance cognition and mood if administered at menopause. While we did not test the long-term effects of MHT in the present study, others have theorized that MHT could reduce the risk of neurodegenerative disorders like Alzheimer disease, but only if initiated shortly after menopause—the “critical window” hypothesis [3,4]. Differences in the timing of MHT initiation could partly explain discrepant findings from prior clinical trials and observational studies. For example, results from trials involving recently postmenopausal women and several large observational studies including women initiating MHT shortly after menopause suggest that MHT has either a neutral or beneficial effect on cognition and mood [5–11]. In contrast, findings from several large studies, including the Women’s Health Initiative Memory Study (WHIMS), enrolling women aged 65 y and older indicated that both opposed and unopposed conjugated equine estrogens (CEE) were associated with adverse cognitive effects [12–17] and no mood benefits [16,17].
The Kronos Early Estrogen Prevention Study–Cognitive and Affective Study (KEEPS-Cog), an ancillary study of the Kronos Early Estrogen Prevention Study (KEEPS) [18–20], is a randomized trial funded by the US National Institutes of Health-Institute on Aging (NIH-NIA) designed to characterize the cognitive and mood effects of up to 4 y of MHT in recently postmenopausal women. The primary Kronos Early Estrogen Prevention Study (KEEPS) was designed to test the effects of early initiation of oral or transdermal MHT versus placebo on a surrogate measure of atherosclerotic progression, carotid artery intima-media thickness. Unique features of the KEEPS include exclusive enrollment of a large sample of recently postmenopausal women, within 3 y of their last menstrual period (LMP); evaluation of the efficacy of a low dose of oral CEE (o-CEE) and transdermal estradiol (t-E2) in a single study; cyclical administration of oral micronized progesterone (m-P; Prometrium); and examination of the effects of MHT on cognition and mood and related symptoms in non-depressed recently postmenopausal women.
Depending on the formulation and mode of delivery, MHT may exert differential cognitive and mood effects [21,22]. Among the key differences between t-E2 and o-CEE are the “first pass” hepatic metabolism occurring with oral estrogens before the drug reaches systemic circulation, and variations in the predominant form of estrogen in each preparation (17β estradiol in the transdermal product versus estrone in CEE [21,22]). We hypothesized that women randomized to t-E2 but not o-CEE would exhibit cognitive and mood improvements compared to women on placebo. Additionally, we explored the role of a genetic polymorphism potentially influencing response to MHT, apolipoprotein E (APOE) ε4 carrier status. Possessing one or two copies of the ε4 allele confers an increased risk for Alzheimer disease [23], and may influence estrogen’s effects on cognitive and mood outcomes [24].
Presented here are findings from the KEEPS-Cog. Building on findings in women initiating MHT during or shortly after the menopausal transition [5–11], the KEEPS-Cog tested the hypothesis that up to 4 y of MHT would improve cognition and mood when initiated in healthy recently postmenopausal women.
Methods
Design Overview
Women enrolled in the KEEPS [18–20], a randomized, placebo-controlled, double-blind trial, were approached for participation in the KEEPS-Cog. A description of the KEEPS’s recruitment and screening methods, inclusion/exclusion criteria, and participating sites was published previously [18–20]. The KEEPS-Cog was designed to evaluate the potential effects of up to 4 y of t-E2 or o-CEE therapy with cyclical m-P on cognitive and mood outcomes in healthy, non-hysterectomized recently postmenopausal women. The original protocol entailed 5 y of treatment. This was altered in the first year of the study, after reconsideration of study design. Specifically, analyses suggested that the length of follow-up could be shortened without compromising the power to detect changes in study outcomes.
The University of Wisconsin–Madison served as the coordinating center for KEEPS-Cog. Cognitive and mood data were collected at nine US sites. The research team based in Madison, Wisconsin, coordinated data collection, trained study personnel, ensured adherence to the KEEPS-Cog study protocol, and monitored data quality.
Ethical Approval
All participants provided written informed consent. Institutional review boards (IRBs) at the participating sites and the University of Wisconsin approved study procedures. Specifically, the Western Institutional Review Board reviewed and approved activities led by the central KEEPS investigators and Phoenix KEEPS study site investigators. Central KEEPS and Phoenix protocol numbers were as follows: IRB—1058663, Western Institutional Review Board—20040792KEEPS, #10–02980, and MDBHAS #11–05383. The University of Wisconsin Health Science IRB reviewed and approved activities led by the KEEPS-Cog investigators (IRB number: H-2005-0059). Specific study site IRB approvals were obtained from the following institutions: Brigham and Women’s Hospital (IRB number: 2004-P-002144 BWH), Mayo Clinic (IRB number: 2241–04), Columbia University (IRB number: AAAA-8062), Yale University (IRB number: 0409027022), University of Utah (IRB number: 13257), Albert Einstein College of Medicine–Montefiore (IRB number: 04-08-213), University of California, San Francisco (IRB number: 10–02980), and University of Washington (UW IRB number: 26702 and VAPSHCS IRB number: 01048).
Setting and Participants
The KEEPS used print and radio advertisements to recruit and enroll 727 women; of these, 693 (95.3%) provided written informed consent for participation in the KEEPS-Cog. Thirty-four women from the full sample were ineligible, either because they had started study medications prior to the start of the ancillary study (n = 4) or because they declined to participate in the optional cognitive and mood assessments (n = 30). Enrollment occurred between August 2005 and July 2008, with final visits completed in 2012. Fig 1 depicts the number of women screened, enrolled, and followed. Entry into the KEEPS was limited to women in the late menopausal transition and early postmenopausal periods, defined as (1) being within 6–36 mo of their LMP and (2) having a plasma follicle stimulating hormone level of ≥35 ng/ml or serum estradiol level of ≤40 pg/ml. Additional eligibility criteria for the KEEPS involved risk for cardiovascular disease (CVD) (as determined by limits for baseline coronary artery calcium score), body mass index (BMI), blood pressure, fasting total cholesterol and glucose levels, and tobacco use [18–20]. Women were excluded if they had a history of severe psychiatric illness, including untreated major depression, but were allowed to enroll if they were taking anti-depressant medications to manage mild to moderate mood symptoms. If using MHT when enrolled, participants completed a 90-d washout period before study randomization.

In addition to meeting inclusion criteria for entry into the KEEPS [20], women in the KEEPS-Cog were cognitively healthy and free of clinical depression. Screening measures included the Mini-Mental State Examination (MMSE) [25] and Beck Depression Inventory, 2nd edition (BDI-II) [26]. For entry into the KEEPS-Cog, participants’ MMSE scores needed to be above age-, education-, ethnicity-, and race-adjusted cutoff scores suggestive of cognitive impairment [27–29]. To be inclusive, five women whose MMSE scores were below the typical cutoff of 24 of 30 points were included in analysis. For these women, MMSE scores were ≥22 and were determined to be related to language or educational differences rather than impaired cognition. To exclude women with clinical depression, women with screening BDI-II scores that exceeded 28/63 (the cutoff score for severe depression [26]) were excluded.
Randomization and Interventions
Women were randomized in a ratio of 4 : 4:5, favoring placebo. A random number generator (Excel, Microsoft) was used to devise a randomization series, sequenced in blocks of 13. Two individuals, an unblinded officer at the KEEPS coordinating site and a study pharmacist, were aware of the treatment assignment; neither were study investigators. The randomization key was not available to study personnel. The order of randomization was incorporated into a KEEPS database, so that treatment allocation occurred when a study identification number was assigned.
Participants received (1) o-CEE (0.45-mg tablet daily) plus cyclical m-P (200-mg capsule daily for 12 d) and a placebo skin patch, (2) t-E2 (50-μg/d) plus cyclical m-P (200-mg capsule daily for 12 d) and a placebo tablet, or (3) all placebos (a placebo capsule, placebo tablet, and placebo patch). All women were asked (1) to take a study tablet from one bottle, once daily, (2) to take a capsule once daily from the second bottle for the first 12 d of each month, and (3) to apply a new study patch weekly.
KEEPS-Cog procedures were performed in conjunction with the parent study visits. Parent study visits occurred every 3 mo; cognitive and mood data were collected at four of the parent study visits: baseline, and months 18, 36, and 48. At the month 18 and 48 visits, cognitive and mood assessments occurred between days 12 and 30, when women took estrogen preparations (i.e., t-E2 or o-CEE) or matching placebos without m-P. To explore possible effects associated with administration of m-P, the month 36 assessment occurred during the first 12 d of the month, when women were taking both estrogen and progesterone, or corresponding placebos. Sample size estimates performed during study development suggested that allocation of 150 women per group would be adequate to detect differences in outcomes between groups.
Primary Outcomes and Follow-Up
Primary outcomes were grouped into two categories: cognition and mood. Cognition was estimated with a global cognitive measure and four domain scores. Global cognition was evaluated with the Modified Mini-Mental State (3MS) examination [30], a 100-point expanded version of a widely used test, the MMSE [25]. The 3MS exam measures orientation, auditory registration, working memory, recall, language, and constructional skills consistent with the MMSE, and includes questions assessing personal information, verbal fluency, abstraction, and long-term recall. This test was selected for inclusion because it was the primary cognitive assessment used in the WHIMS [12–14].
In addition to measuring global cognition with the 3MS exam, we derived cognitive domain scores from a comprehensive battery of 11 cognitive tests that were summarized with factor analysis. In brief, we began the analysis with a total of 25 subscales (from 13 tests), and after iteratively examining competing models and overall fit, 17 subscales were selected for inclusion in the final factor analysis. Scores from subscales with a restricted distribution were excluded from the factor analysis. Ultimately, subscales from 11 of the 13 tests were included in the four factors. Tests and subscales included in the factors are as follows: (1) California Verbal Learning Test, 2nd edition [31], as administered in the Women’s Health Initiative Study of Cognitive Aging (WHISCA) [16,17]; (2) New York University Paragraph Recall [32]; (3) Benton Visual Retention Test [33]; (4) Controlled Oral Word Association Test–Phonemic Fluency [34]; (5) Controlled Oral Word Association Test–Category Fluency [34]; (6) Trail Making Test A [34]; (7) Trail Making Test B [34]; (8) Stroop Color Word Interference Test [35]; (9) Wechsler Adult Intelligence Scale, 3rd edition (WAIS-3) Letter-Number Sequencing [36]; (10) Wechsler Memory Scale, 3rd edition (WMS-3) Digit Span [37]; and (11) WAIS-3 Digit Symbol [36].
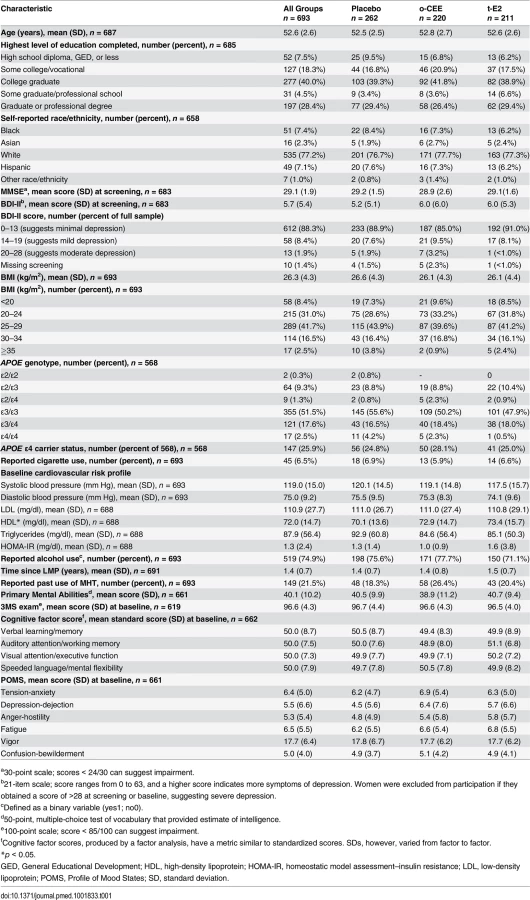
Fig 2 depicts the resultant four cognitive factors: verbal learning/memory, auditory attention/working memory, visual attention/executive function, and speeded language/mental flexibility. Baseline values for the cognitive factors, expressed as T-scores are provided in Table 1. By using multiple scores, summarized as factors, as opposed to individual test scores, we derived more reliable outcomes; the higher the reliability, the greater the power to detect true differences [38]. A full description of the cognitive battery, factor analysis, and summary scores is provided elsewhere [39].

The Profile of Mood States (POMS) [40] was used to examine potential treatment effects of MHT on specific affective states. In this questionnaire, women were asked to rate 65 adjectives using a five-point Likert scale to indicate the agreement between the adjective and their mood over the last week. Scores are summarized into six subscales. Validated as a measure of mood in postmenopausal women [41], the POMS was designed for use with non-depressed populations and is sensitive to subclinical variations in mood states. All six POMS subscales—tension-anxiety, depression-dejection, anger-hostility, fatigue, vigor, and confusion-bewilderment—were included in the analysis.
Other Measures
The BDI-II [26] was used to screen for severe depression prior to enrollment and to monitor for adverse effects over the course of the study. The BDI-II is a 21-item inventory measuring attitudes and symptoms characteristic of depression. Participants were asked to select one of four statements for each symptom item, describing how they felt over the past 2 wk. Zero indicated the absence of a symptom; the numbers one through three corresponded to increasing symptom severity. A total score representing a sum value of responses was derived.
Statistical Analysis
In the modified intent-to-treat analysis, participants with the baseline assessment and at least one post-baseline assessment were included in analyses in their original randomization group, regardless of drop-in or drop-out status in the parent KEEPS. Outcomes were selected based on their likelihood to detect group differences in response to MHT. Based on the number of women enrolled in the parent KEEPS, we expected a final sample size of 150 women per group, assuming an estimated 75% of women would be willing to participate in the ancillary KEEPS-Cog and an anticipated attrition rate of 4% per year. With 150 women per group, original power estimates suggested >80% power to detect group differences for the various outcome measures.
To examine the effect of treatment on cognition and mood throughout the study duration, MHT effects were analyzed using a linear mixed-effects (LME) [42] modeling approach; randomization group functioned as the grouping factor, and time since baseline functioned as a discrete fixed factor. Assuming that data are not missing due to systematic factors, LME models make full use of all available data from each participant [43], in contrast to models excluding participants with partial data.
To test the assumption that data were missing due to random factors, we compared the distribution of baseline variables in Table 1 for participants who completed the study and participants who were lost to follow-up. We also examined the pattern of missing data across variables, in order to detect possible patterns in the distribution of missing values related to various subgroup characteristics (e.g., age, race), and data appeared to be missing in a random manner. Additionally, LME model assumptions about linearity, normality, and the independence and homoscedasticity of errors were assessed graphically and analytically. Linear associations between predictors (treatment group) and cognitive and mood outcomes were verified by adding a quadratic term to models, and evaluating model fit. Treatment assignments were balanced by site; however, to address possible systematic differences in participants related to enrollment site, we included testing site as a random effect in all models. Age and education level were entered as fixed effects covariates, adjusting for baseline individual differences. Finally, for all models, the time factor included discrete values representing months elapsed since baseline, i.e., 0, 18, 36, and 48 mo. The fitted models are available in S3 Text.
The estimates provided by the LME models represent the interaction of time by treatment group (t-E2 and o-CEE), using the placebo group as reference. Our primary interest was to compare the effect of MHT versus placebo (t-E2 versus placebo and o-CEE versus placebo) on changes in cognitive performance and mood across time (where time represents months since baseline) after controlling for baseline age and education level. To determine the magnitude of the effects, we calculated an effect size (ES) by dividing the regression coefficient estimate by the baseline standard deviation of the outcome measures. The length of the study in a month metric was used to adjust the estimate. The estimate of ES can be interpreted as a Cohen’s d effect [44].
Our analyses of cognition and mood outcomes were performed separately, using the same analytic approach and p-value of 0.05, so that women with only one set of data could be included in the appropriate analysis. For example, mood analyses included data from the subset of women who provided data for the POMS outcomes, whether or not they provided data on the cognitive outcomes. To correct for multiple comparisons, we divided the p-value by the number of outcomes. For example, there were five cognitive outcomes (four domain factors and one global cognition score) and six POMS mood scores. Splitting the significance value of 0.05 equally between the five cognitive and six mood sub-domains resulted in a p-value of 0.01 for each of the two primary domains investigated (cognition and mood). We used the statistics software package R, version 2.13 (R Development Core Team; http://cran.r-project.org/), to explore the longitudinal data and model assumptions and SAS, version 9.3 (SAS Institute), to estimate the model parameters.
Prespecified secondary analyses examined the influence of participant characteristics and co-administration of m-P on MHT response. For example, the influence of APOE ɛ4 genotype, a genetic risk factor for dementia [23], on cognitive and mood outcomes was evaluated by adding a dichotomous variable (ɛ4 positive versus ɛ4 negative) to cognitive and mood outcome models as a moderator. The influence of time since LMP was examined in a model by adding in a continuous variable depicting time in months since LMP. In brief, we modeled the interaction of time since LMP by treatment group (o-CEE or t-E2), with placebo group as the reference. The effect of baseline mood as a moderator of cognitive response to MHT was also explored, using baseline BDI-II score in models examining cognitive effects over time. Baseline BDI-II score was evaluated as a continuous variable in models comparing the interaction of baseline BDI-II score by treatment group (o-CEE or t-E2), using the placebo group for reference in each model. Finally, to evaluate the effects of co-administration of m-P on cognitive and mood outcomes, change from baseline score obtained at month 36 was compared to change from baseline score obtained at month 48. Unlike other visits, month 36 assessments occurred during the first 12 d of the month, when women were taking combined estrogen and m-P or corresponding placebos.
Results
The baseline characteristics of the 693 women who completed either cognitive testing or the POMS are presented by treatment group in Table 1. On average, participants were 52.6 y old and 1.4 y past their LMP at baseline. At screening, 71 (10.4%) of the 683 women for whom screening BDI-II scores were available reported symptoms suggestive of mild or moderately severe depression, although none were diagnosed with clinical depression; 58 women scored in the mildly depressed range (14 to 19 out of 63 points), and 13 women scored as having moderate depressive symptoms (20 to 28 out of 63 points). Consistent with published literature [45], the most common APOE allele was ɛ3 among 568 women genotyped, representing 78.8% of pooled alleles, while the ɛ4 allele represented 14.4% of the pooled alleles. Except for a small difference in serum high-density lipoprotein cholesterol levels, there were no statistically significant baseline differences detected among treatment groups in any of the variables measured. Overall, 34 women who participated in the KEEPS did not enroll in the KEEPS-Cog, and the KEEPS-Cog and KEEPS samples were similar in characteristics. In particular, cardiovascular risk profiles, smoking status, demographics, and past MHT profiles were highly consistent [19].
The number of women reporting a reduction in menopausal symptoms was similar in the KEEPS-Cog and the KEEPS. For example, in the KEEPS-Cog, vasomotor symptoms were common at baseline, with >40% of women reporting moderate to severe hot flashes. All women described a reduction in symptoms 6 mo after initiating study medications; however, women randomized to o-CEE and t-E2 demonstrated a statistically significantly greater reduction in symptoms, e.g., 28.6% of women in the placebo group described moderate to severe hot flashes at month 6, compared to 4.3% of women randomized to o-CEE and 6.7% of women randomized to t-E2. Overall, hot flashes were similarly controlled in the two MHT groups (see S1 Table). Notably, group differences in symptoms attenuated over time as hot flashes abated spontaneously for women in the placebo group.
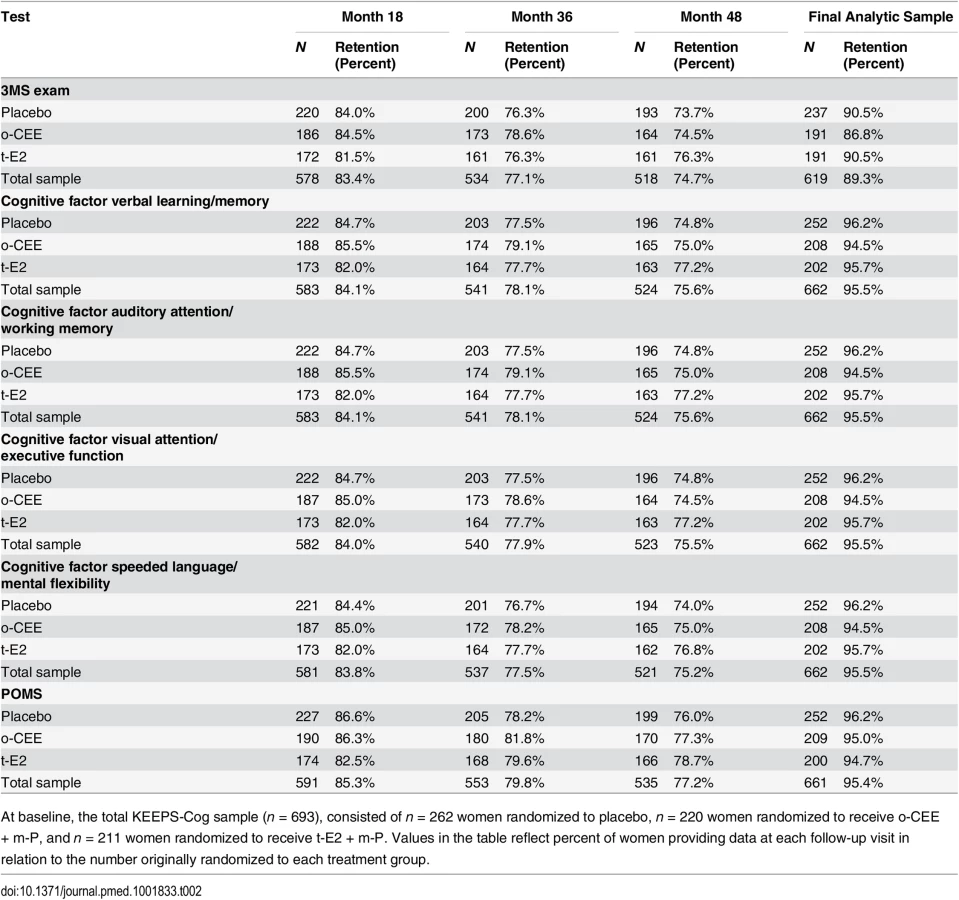
Retention rates by visit and outcome are provided in Table 2. Women completing the baseline visit and at least one post-baseline visit were included in analyses. A total of 662 women were included in the final analytical sample for cognitive factors, and 619 for analysis of 3MS scores. The analyses of POMS outcomes included data from 661 women. The mean follow-up was 2.85 y (SD = 0.49) for cognitive outcomes and 2.76 y (SD = 0.57) for mood outcomes. Harman et al. [20] provide a full summary of adverse events and study withdrawal by randomization group for the KEEPS. For the KEEPS-Cog, 63 serious adverse events occurred in 56 women, 21 of whom were randomized to the o-CEE group, 17 to the t-E2 group, and 18 to the placebo group. Altogether, six cases of breast cancer occurred in women enrolled in the KEEPS-Cog (three in the o-CEE group, two in the t-E2 group, and one in the placebo group). Six women in the KEEPS-Cog experienced cardiac or cerebrovascular events. Specifically, in the o-CEE group, one woman experienced a transient ischemic attack. In the t-E2 group, one woman reported a suspected stroke (later determined not to be a stroke). Two cases of venous thrombotic disease occurred (one in the t-E2 group and one in the placebo group). Two women on o-CEE experienced a major depressive episode. No women developed a cognitive disorder while in the study.
Cognitive Outcomes
Global cognitive performance over time, as measured with the 3MS score, did not differ between treatment groups. Similarly, models investigating MHT effects on the four cognitive factors were also statistically nonsignificant for each active treatment arm versus placebo. Table 3 includes the beta estimates and corresponding p-values for cognitive outcomes by treatment group.

Mood Outcomes
Analysis of POMS scores revealed statistically significant findings (Table 3). Women treated with o-CEE demonstrated improvements over time in POMS tension-anxiety and depression-dejection scores compared to women receiving placebo. Based on a conservative alpha level of 0.01, the anger-hostility index p-value (p = 0.018) was statistically nonsignificant. As listed in Table 3, the beta estimate for the effect of treatment group (o-CEE versus placebo) on linear change over time on the POMS depression-dejection subscale was −5.36 × 10−2 (ES = 0.49, p < 0.001). That is, treatment was a significant predictor of linear improvements in POMS depression-dejection score. The beta estimate associated with o-CEE suggests a medium ES for the improvement in depression-dejection score relative to placebo. The ES for the statistically significant difference on the POMS tension-anxiety subscale with o-CEE was in the small to medium range: −3.01 × 10−2 (ES = 0.26, p < 0.001).
Standards for interpreting the clinical significance of POMS score changes were established for clinical trials examining pain control [46]. An expert panel recommended that a change of one standard error of the mean or half of a standard deviation should be considered clinically significant. When normative data are used as the standard, this corresponds to a two - to five-point change on the individual POMS subscales. S4 Text provides additional information, including a table listing the change in raw scores on the POMS subscales at each visit. According to these guidelines, the o-CEE group demonstrated clinically meaningful change at month 48 on the depression-dejection and tension-anxiety subscales and a borderline meaningful change on the anger-hostility subscale.
Compared to placebo, women assigned to receive t-E2 did not show improvement on any POMS subscales. Moreover, neither treatment group differed from placebo on the POMS confusion-bewilderment or fatigue subscales over time (p-values ranged from 0.125 to 0.630).
In a secondary analysis requested at peer review, we found no statistically significant effect of MHT on BDI-II score (S3 Table). Like other comparisons, the models examined performance between groups across treatment duration (i.e., treatment by time interaction).
Prespecified Secondary Analyses
Four secondary analyses explored the influence of APOE ɛ4 carrier status, time since LMP, co-administration of m-P, and baseline depressive symptoms on response to treatment. The inclusion of APOE status (i.e., ɛ4 positive versus ɛ4 negative) did not influence cognitive or affective response to MHT, nor did time since LMP predict response to MHT for either mood or cognitive outcomes. Comparison of cognitive and mood outcomes obtained at visits occurring either during co-administration of estrogens and m-P (month 36) or during administration of estrogens alone (month 48) revealed no statistically significant differences, suggesting no overt cognitive or mood effects of m-P.
To explore whether baseline depression moderated the cognitive effects of MHT, baseline BDI-II score was entered into the model as a continuous variable, and its interaction with treatment evaluated. Sixty-four (10.0%) of the 637 women for whom both baseline BDI-II scores and cognitive factor scores were available reported symptoms suggestive of mild or moderately severe depression, although none were diagnosed with clinical depression; 52 women scored in the mildly depressed range (14 to 19 out of 63 points), and 12 women scored as having moderate depressive symptoms (20 to 28 out of 63 points). The results of this analysis were nonsignificant. For example, parameter estimates for women treated with o-CEE whose BDI-II scores suggested mild to moderately severe symptoms of depression at baseline, compared to women on placebo, were as follows: 5.65 × 10−4 for the auditory attention/working memory factor (p = 0.08) and 6.50 × 10−4 for the visual attention/executive function factor (p = 0.09). Of note, the range of mood symptoms as measured with the BDI-II was restricted in that women with scores indicative of severe depression were excluded from the study at screening. Findings from these planned secondary analyses were considered exploratory.
Discussion
The KEEPS-Cog is, to our knowledge, the first large randomized clinical trial designed to examine cognition and mood effects for up to 4 y of two forms of MHT therapy in healthy, non-hysterectomized women in late menopausal transition and the early postmenopausal period (i.e., within 36 mo of LMP). Findings demonstrated that treatment with o-CEE resulted in statistically significant reduction in symptoms of tension-anxiety and depression-dejection, corresponding to medium and small to medium ESs, respectively. No mood effects were found for t-E2, and neither form of MHT affected cognition.
Cognitive Effects of Menopausal Hormone Therapy
In this trial, neither MHT formulation affected cognitive function in healthy recently postmenopausal women. Contrary to our hypothesis, treatment with t-E2 did not improve cognition in recently postmenopausal women. The KEEPS-Cog findings are consistent with findings from the Women’s Health Initiative Memory Study of Younger Women (WHIMSY) [2] and a recent meta-analysis [47] suggesting that MHT use in the early postmenopausal period has no cognitive effects. The authors of the WHIMSY trial contrasted their findings to those from the WHIMS and others, which indicated adverse cognitive effects of both opposed and unopposed CEE in older postmenopausal women [12–17]. Together with WHIMSY, the findings from the KEEPS-Cog suggest that MHT is neither deleterious nor beneficial for cognition in younger women. Conflicting results of the WHIMS and others [12–17] and the WHIMSY [2] and KEEPS-Cog are likely due to study design differences discussed below.
Oral Conjugated Equine Estrogens Improved Mood
The effects found in this trial are supported by previous studies [21] and results demonstrating that estrogens and progestins favorably influence neurotransmitters involved in mood regulation, including serotonergic and noradrenergic systems [48]. Similarly, our findings were highly consistent with results from a meta-analysis of clinical studies—the majority of which used o-CEE [49]—that found that MHT with or without progesterone exerts beneficial effects on mood during the menopausal transition and early postmenopausal periods, with a medium ES of 0.45.
In the Study of Women’s Health Across the Nation (SWAN), women experienced an increase in affective symptoms during menopause, and were two to four times more likely to experience depression during the menopausal transition compared to the premenopausal stage ([50,51]). Several studies report an increased incidence of affective symptoms during the menopausal transition [50–54]. Moreover, plasma E2 levels are lower among depressed women [55], suggesting that low estrogens may be associated with mood disorders. In contrast, women in the KEEPS-Cog who were in the late menopausal transition or early postmenopausal period and treated with o-CEE demonstrated improved depression and anxiety symptoms over women on placebo.
In comparison, studies involving CEE, with or without medroxyprogesterone (MPA), in women a decade or more past the menopausal transition [16,17] reported neutral effects of MHT on mood as assessed by general measures of mood [56]. The WHISCA findings together with those from the KEEPS-Cog suggest that CEE-mediated improvements in mood may occur only in recently postmenopausal women and women transitioning to postmenopause. Consequently, the effects of MHT on mood might be most relevant for symptoms occurring during or immediately after menopause [57,58]―a period when women exhibit a particular vulnerability for depression [50,51,59]. Still, it must be acknowledged that these potentially beneficial effects were found only in a subset of POMS outcomes, and ESs were in the medium and small to medium ranges. Moreover, mood effects were detected with the POMS and not the BDI-II. The two tests differ in that the POMS is sensitive to subclinical variations in multiple mood states, whereas the BDI-II assesses symptoms associated with major and minor depression. The BDI-II was included to monitor for major depressive episodes: an analysis of treatment effects on depression as measured with the BDI-II revealed no statistically significant differences between groups.
In contrast to the present findings for o-CEE and previous findings for t-E2 [7], therapy with t-E2 did not improve mood in the KEEPS-Cog. Although the potential mechanisms underlying these findings are currently unclear, and our findings offer only indirect comparisons, it is possible that differences in o-CEE and t-E2 formulations could account for the discrepancy. Results from the KEEPS confirm that women randomized to t-E2 and o-CEE demonstrate divergent estradiol and estrone profiles while on study medications [20]. Compared to placebo, women randomized to receive o-CEE demonstrated markedly increased levels of estrone, and small but statistically significant increases in estradiol levels at months 12, 36, and 48. In contrast, women receiving t-E2 exhibited statistically significant increases in estradiol, and small but statistically significant elevations in estrone levels at the same time points. Additionally, compared to estradiol, CEE is associated with higher levels of estrone sulfate, as well as many other metabolic products, the neurobiology of which are essentially unknown [60]. Only a direct comparison of the two formulations would address whether differential cognitive and mood efficacies exist. Indeed, other studies suggest that various CEE hormones exert differential degrees of neuroprotection [61,62] and that beneficial neuronal effects may be achieved by combining human and nonhuman hormones [61].
Timing of Initiation of Hormone Therapy
Evidence from prospective cohort as well as laboratory studies supports the “critical window” hypothesis. Recent findings from the Cache County Study [1], a prospective cohort study of women starting unopposed MHT within 5 y of menopause, reported a reduced risk for Alzheimer disease compared to those initiating therapy beyond early menopause and compared to women who used opposed MHT. Similarly, results from several laboratory and animal studies that generated the “healthy cell bias” hypothesis [63–66] also support the critical window hypothesis by demonstrating that estrogens protected only non-diseased cells. Unlike the WHIMS and WHISCA [12–14,16,17], the KEEPS-Cog exclusively enrolled recently postmenopausal women, all of whom were cognitively and physically healthy.
Forms and Administration of Progesterone
In the KEEPS-Cog, participants on active estrogens received cyclic m-P, a compound identical to endogenous progesterone, rather than a continuous MPA, as in the Women’s Health Initiative studies. Several studies point to adverse neurobiological and clinical effects of MPA on cognition and mood [67–70]. Moreover, while MPA is androgenic, there is evidence that m-P exerts multiple neuroprotective effects in the brain [70]. Supporting evidence from a small randomized, controlled trial suggested that CEE + m-P, but not CEE + MPA, improved cognition in recently postmenopausal women [71]. While the present study found no cognitive or mood effects of co-administration of estrogen and m-P compared to estrogen alone, the KEEPS-Cog design provided only a cursory examination of the potential effects of m-P.
Limitations
The KEEPS-Cog results cannot be extrapolated to treatment extending beyond 4 y. This limitation is noteworthy because extended therapy is associated with elevated risks for adverse events, depending upon the formulation of MHT used and the health status of the woman at the time MHT is initiated. While some observational studies report prolonged beneficial effects of MHT initiated early in menopause [1,9–11], evaluation of women years after participation in MHT trials revealed a range of effects on cognitive and neuroimaging outcomes [2,72–74].
It is possible that women were aware of their treatment assignment due to reductions in menopausal symptoms. Indeed, between 80% and 90% of women assigned to the o-CEE and t-E2 groups accurately guessed that they were receiving MHT (see S2 Table); still, only women in the o-CEE group demonstrated improved mood, making it unlikely that the improvements in mood were related solely to reductions in menopausal symptoms or to inadvertent unblinding.
Several factors limit the study’s generalizability. Women in the KEEPS were predominantly white, generally well-educated, and at low risk for CVD. Thus, while KEEPS participants were not fully representative of the general postmenopausal US population, they may define a group of women for whom MHT would be appropriate. Additionally, hysterectomized women were excluded from the trial; thus, the findings may not apply to hysterectomized women.
Another limitation of the KEEPS-Cog is that it was neither large enough nor of sufficient duration to assess clinical events such as dementia; rather, the KEEPS-Cog was designed to detect changes in markers of cognitive and mood outcomes, arguably of less importance than incidence of clinical diagnoses. Finally, while a conservative p-value was selected to account for multiple comparisons, the possibility of type-1 error still exists.
Conclusions
The results of the KEEPS-Cog demonstrate that MHT did not improve cognition when initiated in healthy recently postmenopausal women compared to placebo. For mood outcomes, administration of low-dose o-CEE for up to 4 y was associated with statistically significant improvements in symptoms of anxiety and depression, mood symptoms commonly seen in recently postmenopausal women; however, administration of t-E2 did not benefit mood. The statistically significant findings associated with o-CEE administration corresponded to small to medium ESs.
It is notable that neither MHT regimen altered cognition. In other words, results did not indicate adverse or beneficial cognitive effects associated with MHT. The divergent affective findings for o-CEE and t-E2 formulations are interesting, and perhaps expected, given the formulations’ differential chemical composition, mode of access to the systemic circulation, and binding affinity of the ligands for estrogen receptors. Importantly, the KEEPS-Cog finding that o-CEE and not t-E2 was associated with improved mood is contrary to our hypothesis. Additional studies directly comparing the long-term effects and mechanisms of action of these two formulations is warranted.
In total, we propose that the findings of the KEEPS and the KEEPS-Cog could be incorporated into clinical decisions for cardiovascularly healthy, non-hysterectomized women considering whether or not to use MHT. For example, a woman considering MHT for management of menopausal symptoms, including vasomotor, cognitive, and mood concerns, could be informed that MHT will not address her cognitive symptoms. Moreover, while various forms of MHT address vasomotor symptoms, not all MHTs demonstrate improvements in mood outcomes over placebo. She may also be reassured that time-limited MHT use around the age of menopause does not appear to have deleterious cognitive effects such as those observed in the older women enrolled in the WHIMS [12–14]. Finally, discussions of the risks associated with MHT, for example, the risk for breast cancer associated with extended therapy, must be considered alongside the benefits for mood and vasomotor symptoms. While limited, preliminary data suggest that use of low-dose MHTs for a brief period of time may be associated with a lower risk for breast [75] and endometrial [76] cancers. The effects of low-dose and brief MHT on CVD risk factors are mixed [77,78] compared to traditional doses of MHT. Overall, the KEEPS [20] may provide some of the most comprehensive safety data for two low-dose MHTs used for brief duration. Further examination is needed, especially considering the variations in dose, hormone formulation, and route of administration used in studies examining the safety profile of low-dose estrogens.
Together with her health care provider, a woman experiencing problematic symptoms around her menopausal transition can weigh the known risks of MHT against potential benefits for her unique symptom profile, and make an informed decision as to whether she would benefit from MHT, or whether she would prefer to manage symptoms through other means. Overall, the KEEPS-Cog findings provide valuable information to women considering the various options for managing menopausal symptoms.
Supporting Information
Zdroje
1. Shao H, Breitner JC, Whitmer RA, Wang J, Hayden K, Wengreen H, et al. Hormone therapy and Alzheimer disease dementia: new findings from the Cache County Study. Neurology. 2012;79 : 1846–1852. doi: 10.1212/WNL.0b013e318271f823 23100399
2. Espeland MA, Shumaker SA, Leng I, Manson JE, Brown CM, Leblanc ES, et al. Long-term effects on cognitive function of postmenopausal hormone therapy prescribed to women aged 50 to 55 years. JAMA Intern Med. 2013;173 : 1429–1436. 23797469
3. Resnick SM, Henderson VW. Hormone therapy and risk of Alzheimer disease: a critical time. JAMA. 2002;288 : 2170–2172. 12413378
4. Sherwin BB. Estrogen and memory in women: how can we reconcile the findings? Horm Behav. 2005;47 : 371–375. 15708768
5. Joffe H, Hall JE, Gruber S, Sarmiento IA, Cohen LS, Yurgelun-Todd D, et al. Estrogen therapy selectively enhances prefrontal cognitive processes: a randomized, double-blind, placebo-controlled study with functional magnetic resonance imaging in perimenopausal and recently postmenopausal women. Menopause. 2006;13 : 411–422. 16735938
6. Sherwin B. Estrogen and/or androgen replacement therapy and cognitive functioning in surgically menopausal women. Psychoneuroendocrinology. 1988;13 : 345–357. 3067252
7. Sherwin B. Affective changes with estrogen and androgen replacement therapy in surgically menopausal women. J Affect Disord. 1988;14 : 177–187. 2966832
8. Soares CN, Almeida OP, Joffe H, Cohen LS. Efficacy of estradiol for the treatment of depressive disorders in perimenopausal women: a double-blind, randomized, placebo-controlled trial. Arch Gen Psychiatry. 2001;58 : 529–534. 11386980
9. Kawas C, Resnick S, Morrison A, Brookmeyer R, Corrada M, Zonderman A, et al. A prospective study of estrogen replacement therapy and the risk of developing Alzheimer’s disease: the Baltimore Longitudinal Study of Aging. Neurology. 1997;48 : 1517–1521. 9191758
10. Baldereschi M, Di-Carlo A, Lepore V, Bracco L, Maggi S, Grigoletto F, et al. Estrogen-replacement therapy and Alzheimer’s disease in the Italian Longitudinal Study on Aging. Neurology. 1998;50 : 996–1002. 9566385
11. Paganini-Hill A, Henderson VW. Estrogen replacement therapy and risk of Alzheimer disease. Arch Intern Med. 1996;156 : 2213–2217. 8885820
12. Rapp SR, Espeland MA, Shumaker SA, Henderson VW, Brunner RL, Manson JE, et al. Effect of estrogen plus progestin on global cognitive function in postmenopausal women: the Women’s Health Initiative Memory Study: a randomized controlled trial. JAMA. 2003;289 : 2663–2672. 12771113
13. Shumaker SA, Legault C, Rapp SR, Thal L, Wallace RB, Ockene JK, et al. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in postmenopausal women: the Women’s Health Initiative Memory Study: a randomized controlled trial. JAMA. 2003;289 : 2651–2662. 12771112
14. Espeland MA, Rapp SR, Shumaker SA, Brunner R, Manson JE, Sherwin BB, et al. Conjugated equine estrogens and global cognitive function in postmenopausal women: Women’s Health Initiative Memory Study. JAMA. 2004;291 : 2959–2968. 15213207
15. Grady D, Yaffe K, Kristof M, Lin F, Richards C, Barrett-Connor E. Effect of postmenopausal hormone therapy on cognitive function: the Heart and Estrogen/progestin Replacement Study. Am J Med. 2002;113 : 543–548. 12459399
16. Resnick SM, Espeland MA, An Y, Maki PM, Coker LH, Jackson R, et al. Effects of conjugated equine estrogens on cognition and affect in postmenopausal women with prior hysterectomy. J Clin Endocrinol Metab. 2009;94 : 4152–4161. doi: 10.1210/jc.2009-1340 19850684
17. Resnick SM, Maki PM, Rapp SR, Espeland MA, Brunner R, Coker LH, et al. Effects of combination estrogen plus progestin hormone treatment on cognition and affect. J Clin Endocrinol Metab. 2006;91 : 1802–1810. 16522699
18. Miller VM, Black DM, Brinton EA, Budoff MJ, Cedars MI, Hodis HN, et al. Using basic science to design a clinical trial: baseline characteristics of women enrolled in the Kronos Early Estrogen Prevention Study (KEEPS). J Cardiovasc Transl Res. 2009;2 : 228–239. doi: 10.1007/s12265-009-9104-y 19668346
19. Harman SM, Brinton EA, Cedars M, Lobo R, Manson JE, Merriam GR, et al. KEEPS: the Kronos Early Estrogen Prevention Study. Climacteric. 2005;8 : 3–12. 16112947
20. Harman SM, Black DM, Naftolin F, Brinton EA, Budoff MJ, Cedars MI, et al. Arterial imaging outcomes and cardiovascular risk factors in recently menopausal women: a randomized trial. Ann Intern Med. 2014;161 : 249–260. doi: 10.7326/M14-0353 25069991
21. Wharton W, Gleason CE, Miller VM, Asthana S. Rational and design of the Kronos Early Estrogen Prevention Study (KEEPS) and the KEEPS cognitive and affective sub study (KEEPS Cog). Brain Res. 2013;1514 : 12–7. doi: 10.1016/j.brainres.2013.04.011 23603409
22. Wharton W, Gleason CE, Olson SR, Carlsson CM, Asthana S. Neurobiological underpinnings of the estrogen–mood relationship. Curr Psychiatry Rev. 2012;8 : 247–256. 23990808
23. Saunders AM, Strittmatter WJ, Schmechel D, George-Hyslop PH, Pericak-Vance MA, Joo SH, et al. Association of apolipoprotein E allele epsilon 4 with late-onset familial and sporadic Alzheimer’s disease. Neurology. 1993;43 : 1467–1472. 8350998
24. Yue Y, Hu L, Tian QJ, Jiang JM, Dong YL, Jin ZY, et al. Effects of long-term, low-dose sex hormone replacement therapy on hippocampus and cognition of postmenopausal women of different apoE genotypes. Acta Pharmacol Sin. 2007;28 : 1129–1135. 17640473
25. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12 : 189–198. 1202204
26. Beck AT, Steer RA, Brown GK. Manual for Beck Depression Inventory. 2nd ed. San Antonio (Texas): The Psychological Corporation; 1996.
27. Hawkins KA, Cromer JR, Piotrowski AS, Pearlson GD. Mini-Mental State Exam performance of older African Americans: effect of age, gender, education, hypertension, diabetes, and the inclusion of serial 7s subtraction versus “world” backward on score. Arch Clin Neuropsychol. 2011;26 : 645–652. doi: 10.1093/arclin/acr054 21813555
28. Espino DV, Lichtenstein MJ, Palmer RF, Hazuda HP. Ethnic differences in Mini-Mental State Examination (MMSE) scores: where you live makes a difference. J Am Geriatr Soc. 2001;49 : 538–548. 11380745
29. Bravo G, Hebert R. Age - and education-specific reference values for the Mini-Mental and Modified Mini-Mental State Examinations derived from a non-demented elderly population. Int J Geriatr Psychiatry. 1997;12 : 1008–1018. 9395933
30. Teng EL, Chui HC. The Modified Mini-Mental State (3MS) examination. J Clin Psychiatry. 1987;48 : 314–318. 3611032
31. Delis DC, Kramer JH, Kaplan E, Ober BA. California Verbal Learning Test-II. 2nd ed. San Antonio (Texas): The Psychological Corporation; 2000.
32. Kluger A, Ferris SH, Golomb J, Mittelman MS, Reisberg B. Neuropsychological prediction of decline to dementia in nondemented elderly. J Geriatr Psychiatry Neurol. 1999;12 : 168–179. 10616864
33. Benton A, Hamsher Kd, Varney N, Spreen O. Contributions to neuropsychological assessment. New York: Oxford University Press; 1983.
34. Spreen O, Strauss E. A compendium of neuropsychological tests. 2nd ed. New York: Oxford University Press; 1998.
35. Golden C. The Stroop Color and Word Test: a manual for clinical and experimental uses. Chicago: Stoetling; 1978.
36. Wechsler D. Wechsler Adult Intelligence Scale–III (WAIS-3). New York: The Psychological Corporation; 1991.
37. Wechsler D. Wechsler Memory Scales–3rd edition (WMS-3). San Antonio (Texas): The Psychological Corporation; 1997.
38. Nunnally JC, Bernstein IH. Psychometric theory. 3rd ed. New York: McGraw-Hill; 1994.
39. Dowling NM, Gleason CE, Manson JE, Hodis HN, Miller VM, Brinton EA, et al. Characterization of vascular disease risk in postmenopausal women and its association with cognitive performance. PLoS ONE. 2013;8:e68741. doi: 10.1371/journal.pone.0068741 23874743
40. McNair DM, Lorr M, Droppleman LF. POMS manual. San Diego: Educational and Industrial Testing Service; 1992.
41. Wyrwich KW, Yu H. Validation of POMS questionnaire in postmenopausal women. Qual Life Res. 2011;20 : 1111–1121. doi: 10.1007/s11136-011-9846-2 21279447
42. Demidenko E. Mixed models: theory and applications. Hoboken (New Jersey): Wiley; 2004.
43. Bagiella E, Sloan RP, Heitjan DF. Mixed-effects models in psychophysiology. Psychophysiology. 2000;37 : 13–20. 10705763
44. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale: L. Erlbaum Associates; 1988.
45. Bertram L, McQueen MB, Mullin K, Blacker D, Tanzi RE. Systematic meta-analyses of Alzheimer disease genetic association studies: the AlzGene database. Nat Genet. 2007;39 : 17–23. 17192785
46. Dworkin RH, Turk DC, Wyrwich KW, Beaton D, Cleeland CS, Farrar JT, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J Pain. 2008;9 : 105–121. 18055266
47. Hogervorst E, Bandelow S. Sex steroids to maintain cognitive function in women after the menopause: a meta-analyses of treatment trials. Maturitas. 2010;66 : 56–71. doi: 10.1016/j.maturitas.2010.02.005 20202765
48. Halbreich U, Kahn LS. Role of estrogen in the aetiology and treatment of mood disorders. CNS Drugs. 2001;15 : 797–817. 11602005
49. Zweifel JE, O’Brien WH. A meta-analysis of the effect of hormone replacement therapy upon depressed mood. Psychoneuroendocrinology. 1997;22 : 189–212. 9203229
50. Bromberger JT, Kravitz HM, Chang YF, Cyranowski JM, Brown C, Matthews KA. Major depression during and after the menopausal transition: Study of Women’s Health Across the Nation (SWAN). Psychol Med. 2011;41 : 1879–1888. doi: 10.1017/S003329171100016X 21306662
51. Bromberger JT, Schott LL, Kravitz HM, Sowers M, Avis NE, Gold EB, et al. Longitudinal change in reproductive hormones and depressive symptoms across the menopausal transition: results from the Study of Women’s Health Across the Nation (SWAN). Arch Gen Psychiatry. 2010;67 : 598–607. doi: 10.1001/archgenpsychiatry.2010.55 20530009
52. Hardy R, Kuh D. Change in psychological and vasomotor symptom reporting during the menopause. Soc Sci Med. 2002;55 : 1975–1988. 12406465
53. Woods NF, Mariella A, Mitchell ES. Patterns of depressed mood across the menopausal transition: approaches to studying patterns in longitudinal data. Acta Obstet Gynecol Scand. 2002;81 : 623–632. 12190837
54. Paoletti AM, Floris S, Mannias M, Orru M, Crippa D, Orlandi R, et al. Evidence that cyproterone acetate improves psychological symptoms and enhances the activity of the dopaminergic system in postmenopause. J Clin Endocrinol Metab. 2001;86 : 608–612. 11158017
55. Young EA, Midgley AR, Carlson NE, Brown MB. Alteration in the hypothalamic-pituitary-ovarian axis in depressed women. Arch Gen Psychiatry. 2000;57 : 1157–1162. 11115329
56. Radloff LS. The CES-D Scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1 : 385–401.
57. Schmidt PJ, Rubinow DR. Reproductive hormonal treatments for mood disorders in women. Dialogues Clin Neurosci. 2002;4 : 211–223. 22033644
58. Silva I, Naftolin F. Brain health and cognitive and mood disorders in ageing women. Best Pract Res Clin Obstet Gynaecol. 2013;27 : 661–672. doi: 10.1016/j.bpobgyn.2013.06.005 24007951
59. Tangen T, Mykletun A. Depression and anxiety through the climacteric period: an epidemiological study (HUNT-II). J Psychosom Obstet Gynaecol. 2008;29 : 125–131. doi: 10.1080/01674820701733945 18484441
60. Bhavnani BR. Estrogens and menopause: pharmacology of conjugated equine estrogens and their potential role in the prevention of neurodegenerative diseases such as Alzheimer’s. J Steroid Biochem Mol Biol. 2003;85 : 473–482. 12943738
61. Zhao L, Brinton RD. Select estrogens within the complex formulation of conjugated equine estrogens (Premarin) are protective against neurodegenerative insults: implications for a composition of estrogen therapy to promote neuronal function and prevent Alzheimer’s disease. BMC Neurosci. 2006;7 : 24. 16533397
62. Talboom JS, Engler-Chiurazzi EB, Whiteaker P, Simard AR, Lukas R, Acosta JI, et al. A component of Premarin enhances multiple cognitive functions and influences nicotinic receptor expression. Horm Behav. 2010;58 : 917–928. doi: 10.1016/j.yhbeh.2010.09.002 20849857
63. Brinton RD. Investigative models for determining hormone therapy-induced outcomes in brain: evidence in support of a healthy cell bias of estrogen action. Ann N Y Acad Sci. 2005;1052 : 57–74. 16024751
64. Daniel JM, Hulst JL, Berbling JL. Estradiol replacement enhances working memory in middle-aged rats when initiated immediately after ovariectomy but not after a long-term period of ovarian hormone deprivation. Endocrinology. 2006;147 : 607–614. 16239296
65. Nilsen J, Chen S, Irwin RW, Iwamoto S, Brinton RD. Estrogen protects neuronal cells from amyloid beta-induced apoptosis via regulation of mitochondrial proteins and function. BMC Neurosci. 2006;7 : 74. 17083736
66. Simpkins JW, Wang J, Wang X, Perez E, Prokai L, Dykens JA. Mitochondria play a central role in estrogen-induced neuroprotection. Curr Drug Targets CNS Neurol Disord. 2005;4 : 69–83. 15723615
67. Braden BB, Garcia AN, Mennenga SE, Prokai L, Villa SR, Acosta JI, et al. Cognitive-impairing effects of medroxyprogesterone acetate in the rat: independent and interactive effects across time. Psychopharmacology. 2011;218 : 405–418. doi: 10.1007/s00213-011-2322-4 21562760
68. Braden BB, Talboom JS, Crain ID, Simard AR, Lukas RJ, Prokai L, et al. Medroxyprogesterone acetate impairs memory and alters the GABAergic system in aged surgically menopausal rats. Neurobiol Learn Mem. 2010;93 : 444–453. doi: 10.1016/j.nlm.2010.01.002 20074654
69. Singh M. Progesterone-induced neuroprotection. Endocrine. 2006;29 : 271–274. 16785602
70. Singh M, Su C. Progesterone-induced neuroprotection: factors that may predict therapeutic efficacy. Brain Res. 2013;1514 : 98–106. doi: 10.1016/j.brainres.2013.01.027 23340161
71. Sherwin BB, Grigorova M. Differential effects of estrogen and micronized progesterone or medroxyprogesterone acetate on cognition in postmenopausal women. Fertil Steril. 2011;96 : 399–403. doi: 10.1016/j.fertnstert.2011.05.079 21703613
72. Bagger YZ, Tanko LB, Alexandersen P, Qin G, Christiansen C. Early postmenopausal hormone therapy may prevent cognitive impairment later in life. Menopause. 2005;12 : 12–17. 15668595
73. Espeland MA, Tindle HA, Bushnell CA, Jaramillo SA, Kuller LH, Margolis KL, et al. Brain volumes, cognitive impairment, and conjugated equine estrogens. J Gerontol A Biol Sci Med Sci. 2009;64 : 1243–1250. doi: 10.1093/gerona/glp128 19729392
74. Resnick SM, Espeland MA, Jaramillo SA, Hirsch C, Stefanick ML, Murray AM, et al. Postmenopausal hormone therapy and regional brain volumes: the WHIMS-MRI Study. Neurology. 2009;72 : 135–142. doi: 10.1212/01.wnl.0000339037.76336.cf 19139364
75. Samsioe G, Hruska J. Optimal tolerability of ultra-low-dose continuous combined 17beta-estradiol and norethisterone acetate: laboratory and safety results. Climacteric. 2010;13 : 34–44. doi: 10.3109/13697130903480706 20001563
76. Johnson SR, Ettinger B, Macer JL, Ensrud KE, Quan J, Grady D. Uterine and vaginal effects of unopposed ultralow-dose transdermal estradiol. Obstet Gynecol. 2005;105 : 779–787. 15802405
77. Casanova G, Bossardi Ramos R, Ziegelmann P, Spritzer PM. Effects of low-dose versus placebo or conventional-dose postmenopausal hormone therapy on variables related to cardiovascular risk: a systematic review and meta-analyses of randomized clinical trials. J Clin Endocrinol Metab. 2015;100 : 1028–1037. doi: 10.1210/jc.2014-3301 25514104
78. Casanova G, dos Reis AM, Spritzer PM. Low-dose oral or non-oral hormone therapy: effects on C-reactive protein and atrial natriuretic peptide in menopause. Climacteric. 2015;18 : 86–93. doi: 10.3109/13697137.2014.940309 25017924
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2015 Číslo 6
- Alternativní léčebné možnosti u hypercholesterolemie při intoleranci statinů
- Vliv kombinace nutraceutik na remodelaci levé komory srdeční u osob s metabolickým syndromem
- Nutraceutika a jejich ovlivnění mírného kardiometabolického rizika
- Princip účinku medu v léčbě chronických i infikovaných ran
- Superoxidovaný roztok a jeho využití v léčbě ran
Nejčtenější v tomto čísle
- The Mistreatment of Women during Childbirth in Health Facilities Globally: A Mixed-Methods Systematic Review
- The Potential for Reducing the Number of Pneumococcal Conjugate Vaccine Doses While Sustaining Herd Immunity in High-Income Countries
- Mistreatment of Women in Childbirth: Time for Action on This Important Dimension of Violence against Women
- Associations between Potentially Modifiable Risk Factors and Alzheimer Disease: A Mendelian Randomization Study