
The Evolution of the Epidemic of Charcoal-Burning Suicide in Taiwan: A Spatial and Temporal Analysis
Background:
An epidemic of carbon monoxide poisoning suicide by burning barbecue charcoal has occurred in East Asia in the last decade. We investigated the spatial and temporal evolution of the epidemic to assess its impact on the epidemiology of suicide in Taiwan.
Methods and Findings:
Age-standardised rates of suicide and undetermined death by charcoal burning were mapped across townships (median population aged 15 y or over = 27,000) in Taiwan for the periods 1999–2001, 2002–2004, and 2005–2007. Smoothed standardised mortality ratios of charcoal-burning and non-charcoal-burning suicide and undetermined death across townships were estimated using Bayesian hierarchical models. Trends in overall and method-specific rates were compared between urban and rural areas for the period 1991–2007. The epidemic of charcoal-burning suicide in Taiwan emerged more prominently in urban than rural areas, without a single point of origin, and rates of charcoal-burning suicide remained highest in the metropolitan regions throughout the epidemic. The rural excess in overall suicide rates prior to 1998 diminished as rates of charcoal-burning suicide increased to a greater extent in urban than rural areas.
Conclusions:
The charcoal-burning epidemic has altered the geography of suicide in Taiwan. The observed pattern and its changes in the past decade suggest that widespread media coverage of this suicide method and easy access to barbecue charcoal may have contributed to the epidemic. Prevention strategies targeted at these factors, such as introducing and enforcing guidelines on media reporting and restricting access to charcoal, may help tackle the increase of charcoal-burning suicides.
: Please see later in the article for the Editors' Summary
Published in the journal:
. PLoS Med 7(1): e32767. doi:10.1371/journal.pmed.1000212
Category:
Research Article
doi:
https://doi.org/10.1371/journal.pmed.1000212
Summary
Background:
An epidemic of carbon monoxide poisoning suicide by burning barbecue charcoal has occurred in East Asia in the last decade. We investigated the spatial and temporal evolution of the epidemic to assess its impact on the epidemiology of suicide in Taiwan.
Methods and Findings:
Age-standardised rates of suicide and undetermined death by charcoal burning were mapped across townships (median population aged 15 y or over = 27,000) in Taiwan for the periods 1999–2001, 2002–2004, and 2005–2007. Smoothed standardised mortality ratios of charcoal-burning and non-charcoal-burning suicide and undetermined death across townships were estimated using Bayesian hierarchical models. Trends in overall and method-specific rates were compared between urban and rural areas for the period 1991–2007. The epidemic of charcoal-burning suicide in Taiwan emerged more prominently in urban than rural areas, without a single point of origin, and rates of charcoal-burning suicide remained highest in the metropolitan regions throughout the epidemic. The rural excess in overall suicide rates prior to 1998 diminished as rates of charcoal-burning suicide increased to a greater extent in urban than rural areas.
Conclusions:
The charcoal-burning epidemic has altered the geography of suicide in Taiwan. The observed pattern and its changes in the past decade suggest that widespread media coverage of this suicide method and easy access to barbecue charcoal may have contributed to the epidemic. Prevention strategies targeted at these factors, such as introducing and enforcing guidelines on media reporting and restricting access to charcoal, may help tackle the increase of charcoal-burning suicides.
: Please see later in the article for the Editors' Summary
Introduction
The last decade has witnessed an epidemic of suicides by burning charcoal in some Asian countries [1]. The first widely publicised victim died in Hong Kong in November 1998 [1],[2]. She burnt barbecue charcoal in a sealed room to produce high levels of lethal carbon monoxide. Within 5 y this novel method had become the second most commonly used method of suicide in Hong Kong and Taiwan and may have contributed to the rise in overall suicide rates seen in these countries [3],[4]. The rise in use of this method was thought to be triggered by extensive media coverage, which vividly portrayed charcoal burning as an effective, painless, and peaceful way of ending one's life [1],[3],[5]. The new suicide method spread beyond country boundaries [1],[3]; cases have been reported in other parts of Asia including Macau, Japan [1], and Korea [6], and elsewhere in the world [7]. The geographic pattern of the epidemic has not been systematically investigated, although there appears to be an urban–rural difference in incidence in Taiwan [3],[8]. To the best of our knowledge no previous studies have investigated the spatial and temporal pattern of the emergence of a new suicide method.
Different forms of space-time clustering of suicide have been identified in the literature [9]. “Local” clustering refers to occurrences of suicides that group in both space and time: this has been observed mainly in institutional settings such as hospitals, school, or prisons, where victims may be in social contact with each other. Clustering in time more than place is usually associated with media coverage of events such as celebrity suicides that lead to “imitative” suicides [9]. In the case of the charcoal-burning suicide epidemic, where the media influence is thought to be widespread [1],[3], one might predict that there would be little geographic clustering. Alternatively, it is possible that media exposure varies regionally and people living in different areas differ in their susceptibility to media influence; such differences may lead to variation in rates between areas [10]. An improved understanding of the spatial and temporal patterning of charcoal-burning suicide may help identify factors contributing to the epidemic, and thus inform prevention.
This study aimed to investigate the evolution of the epidemic of charcoal-burning suicide over time and across areas in Taiwan, a country with a population of 23 million and large geographic variation in urbanisation. We compared the spatial patterning of charcoal-burning suicides with that of suicides using other methods, and examined the impact of charcoal-burning suicides on secular trends in rural–urban difference in suicide.
Methods
Data
Electronic mortality data files for suicides and undetermined deaths (International Classification of Diseases [ICD-9] codes E950–E959 and E980–E989) in the period 1991–2007 were provided by the Department of Health, Taiwan. Past research shows that suicide mortality is often underestimated and the most commonly assigned cause of death for “missed” suicides is death of undetermined intent (“undetermined death”) [11],[12]. A previous study in Taiwan showed that, in addition to undetermined deaths, deaths certified as accident by pesticide poisoning (ICD-9 code E863) and suffocation (ICD-9 code E913) might also contain “missed” suicides [13], and thus we included these deaths in sensitivity analyses. There is no specific code for charcoal-burning suicide in ICD-9 and therefore cases were identified using the codes E952/E982 (suicide or undetermined death by poisoning using nondomestic gas). A previous study showed that up to 90% of deaths in Taiwan in these categories were charcoal-burning cases: the rest were mostly suicides by car exhaust poisoning [14]. For simplicity of presentation, we referred to deaths coded as E952/E982 as “charcoal-burning suicides” throughout the paper. Suicides and undetermined deaths coded other than E952/E982 were analysed as “non-charcoal-burning” cases.
Mid-year population data for each of the 358 Taiwanese townships (median population aged 15 y or over: approximately 27,000) in each year were obtained from the Demographic Yearbook published by the Ministry of the Interior, Taiwan. Deaths were assigned to each township according to the registered address of residence on the death certificate. We categorised each township as rural or urban on the basis of the urbanisation index developed by the National Health Research Institute, Taiwan [15]. This index was derived from a cluster analysis using data for the year 2000 on five indicators: population density, percentage of population with college or greater educational levels, percentage of population aged 65 y or over, percentage of population working in agriculture, and density of physicians per 100,000 people. Townships are grouped into seven urbanisation levels, with level 1 as the most urban and level 7 as the least (Figure 1A). We categorised townships in levels 1–3 (126 townships, 73% of the population) as urban and those in levels 4–7 (232 townships, 27% of the population) as rural (Figure 1B), in accordance with official statistics that 77% of the residents lived in urban areas in 2000 [16]. Most of the western, plain areas of Taiwan are categorised as urban, with three major metropolitan regions: one in the north (centred around the capital Taipei city), one in the middle (around Taichung city), and one in the south of Taiwan (around Tainan and Kaohsiung cities). Eastern Taiwan is mostly rural and mountainous, with one major city (Hualien city).

Data Analysis
To investigate changes in spatial patterning over time, sex-specific age-standardised rates of suicide and undetermined death by charcoal burning for each township in the periods 1999–2001, 2002–2004, and 2005–2007 were calculated using the world standard population and mapped. Overall and charcoal-burning–specific rates of suicide as well as the proportions of charcoal-burning suicide were also calculated for each category of urbanisation in men and women during the three time periods. Moran's I statistic was used to test for spatial clustering/autocorrelation. I = 0 indicates no autocorrelation, whilst I = 1 suggests strong spatial autocorrelation (i.e., areas with high rates tend to be proximal to other areas with high rates, and areas with low rates to other areas with low rates). The package GeoDa was used to calculate I statistics, allowing for instability of rates due to small numbers of deaths [17],[18]. The p-values for I statistics were derived from a permutation test.
We calculated standardised mortality ratios (SMRs: the ratio of the observed to expected number of deaths) for each township using data for 1999–2007. Expected deaths were calculated by multiplying the national sex - and age-specific suicide rates (in 5-y age-bands) by the corresponding sex - and age-specific population-years at risk in each township. In areas with small populations the small number of deaths can result in unreliable rate estimates. Therefore Bayesian hierarchical Poisson regression models were used to estimate smoothed SMRs for each township, allowing for “global” between-area variability and “local” variability owing to spatial autocorrelation (i.e., neighbouring areas tend to have more similar rates) [19]–[21]. In the study, “neighbours” were defined as the sets of townships that share a border. In models specifying only global variability, the “globally” smoothed SMR is estimated as a weighted average of the observed value and the national mean: the greater the uncertainty in estimating the area SMRs (in sparsely populated regions), the greater the degree of smoothing towards the national mean. In models specifying only local variability, the “locally” smoothed SMR is a weighted average of the observed SMR and the SMRs in neighbouring areas; the greater unreliability in estimating the SMRs, the higher degree of smoothing towards the local mean. Models specifying both global and local variability (convolution models) allow estimation of the relative contribution of each component to the total variability [22].
Smoothed SMRs were estimated using the Markov chain Monte Carlo methods [23] implemented in WinBUGS version 1.4. The built-in conditional autoregressive distribution was used to smooth SMRs towards the local mean [24]. Vague prior distributions were used. Convergence was assessed using the Gelman-Rubin statistic [25], on the basis of four parallel chains, and models were compared on the basis of the deviance information criterion (DIC).
Mapping
Smoothed SMRs for suicide and undetermined death by charcoal burning and by other methods were mapped separately, using five category breaks and a divergent red–blue colour scheme [26]. The chosen categories were symmetrical on the logarithmic scale around the middle category (i.e., SMRs of 0.9–1.1) and presented in red with varying lightness for those higher than the middle category, blue for those lower than the middle category, and white for those that belong to the middle category. Five categories were used because past research suggests that people are able to interpret small maps (sized one-quarter of a standard page) better when five shades of colour are used [26]. ArcGIS Version 9.3 was used to produce the maps. In a sensitivity analysis, we analysed data for people aged 25–44 y only, as this age group has a higher risk of charcoal-burning suicide than others [3],[8],[27].
Secular trends in overall and method-specific (charcoal-burning versus non-charcoal-burning) rates for suicide and undetermined deaths for the period 1991–2007 were examined graphically and compared between rural and urban areas in Taiwan.
Results
Of 53,440 suicides and undetermined deaths in the period 1991–2007, 6,911 (12.9%) were by charcoal burning or other nondomestic gas. The proportion increased from 0.1% in 1991 to 26.6% in 2007. The first charcoal-burning case occurred in Hong Kong in November 1998; during the period 1999–2007, 6,822 (18.7%) of 36,480 suicides and undetermined deaths were by charcoal burning or other nondomestic gas in Taiwan.
The Emergence of the Epidemic of Charcoal-Burning Suicide over Time and across Areas
Figure 2 shows the maps of raw (unsmoothed) age-standardised rates of charcoal-burning suicide in males and females, for the periods 1999–2001, 2002–2004, and 2005–2007. In the early years of the epidemic (1999–2001), charcoal-burning suicides were mainly seen in West Taiwan, mostly but not entirely in urban areas. There was no evidence for a single geographic point of origin for the epidemic. High rates were also seen in a few rural, mountainous townships, but because their populations were small, a small excess of deaths could lead to extreme estimates of rates. In 2005–2007 charcoal-burning suicides were seen in most areas in Taiwan except some of the eastern, rural townships.
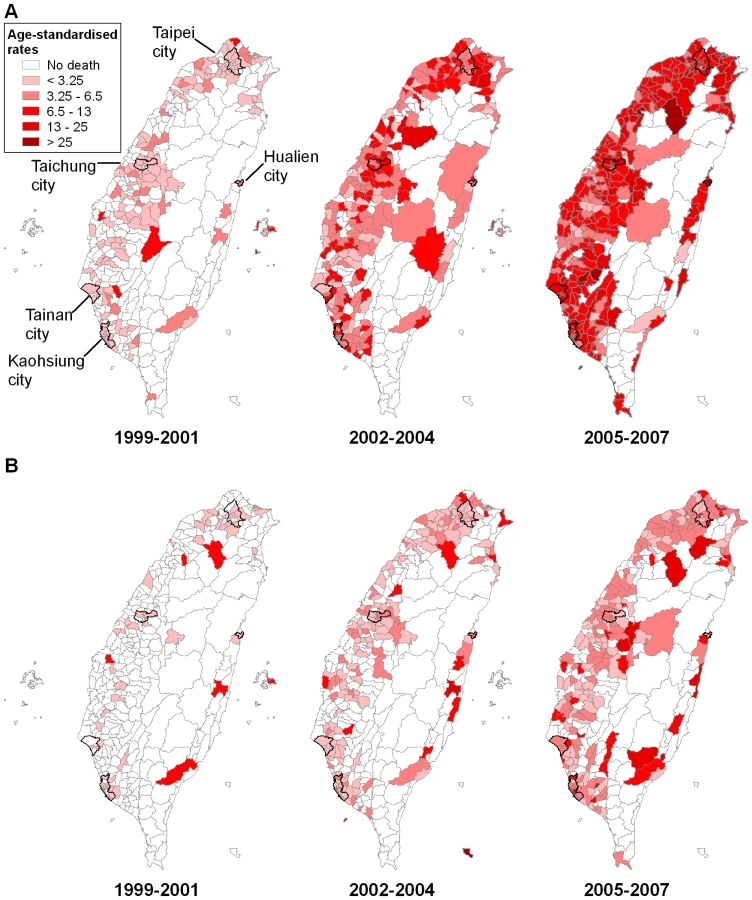
Rates of charcoal-burning suicide were consistently higher in areas with higher levels of urbanisation and higher in men than women throughout the epidemic (Table 1). Overall, there was an urban–rural gradient in both rates and the proportions of charcoal-burning suicide from the early to the most recent years of the epidemic. In women, rates in areas with urbanisation level 5 were low; this category contained the smallest population amongst all levels (2.3% of total population) and thus estimates were unstable.

Spatial Patterning: Charcoal-Burning Versus Non-Charcoal-Burning Suicides
Figure 3 shows the globally and locally smoothed maps of suicides and undetermined deaths by charcoal burning and other methods, for males and females, in the years 1999–2007. There were 4-fold (males) and 10-fold (females) differences in smoothed SMRs for charcoal-burning suicide. Smoothed SMRs ranged from 0.39 to 1.70 (90% range 0.57–1.26) in men and 0.16 to 2.05 (90% range 0.68–1.26) in women. The maps displayed clear evidence of spatial patterning that was similar in men and women; high SMRs for charcoal burning suicides were seen in all three major metropolitan regions of West Taiwan, with the capital Taipei city being somewhat spared, and in the only city of East Taiwan (Hualien). On the basis of the deviance information criterion (DIC), the models accounting for both the global and local variability across areas showed better goodness of fit than models accounting for global variability only, and at least equal fit in comparison to models accounting for local variability only. Therefore we presented the maps of SMRs smoothed both globally and locally here. The models estimated that 89.2% (95% credible interval [CrI] 74.9%–97.4%) of the total area variability in male charcoal-burning suicides could be attributed to the local component, and the corresponding figure for females was 85.0% (95% CrI 59.6%–97.4%), indicating that local characteristics contributed to the majority of the variability of SMRs across townships. Moran's I statistics showed evidence of spatial autocorrelation (I: 0.31 [p = 0.001] for males, 0.11 [p = 0.004] for females).

The spatial patterning of charcoal-burning suicide was little changed when data on deaths aged 25–44 y only were analysed (unpublished data). Analyses on data excluding undetermined deaths also showed similar patterns, except that high SMRs in the middle metropolitan area were less evident (unpublished data). When including accidental deaths from pesticide poisoning and suffocation, the spatial patterns of non-charcoal-burning suicides remained generally the same (unpublished data). Spatial patterns of unsmoothed SMRs were broadly similar to those in the smoothed maps, but the patterns were less clearly displayed because there were no charcoal-burning suicides in many townships (35/358 [9.8%] in men, 101/358 [28.2%] in women) (unpublished data).
Smoothed SMRs for non-charcoal-burning suicides showed less between-area variability than those for charcoal-burning suicides: they ranged from 0.53–1.89 in men (90% range 0.83–1.52) and from 0.70–1.75 in women (90% range 0.86–1.38). Non-charcoal-burning suicides had a completely different spatial distribution compared with charcoal-burning suicides (Figure 3). Rural areas in East Taiwan had higher smoothed SMRs than the western, urban areas.
Secular Trends in Rural–Urban Difference in Suicide
Figure 4 shows secular trends in rates of overall, charcoal-burning and non-charcoal-burning suicide and undetermined death (3-y moving averages) for the period 1991–2007 in urban and rural areas of Taiwan, separately for males and females. Overall suicide rates increased throughout the period, but rural–urban differences changed over time (Figure 4A). In the early 1990s overall suicide rates were higher in rural than urban areas; the differences widened in the mid-1990s in men but narrowed markedly after 2000 in both men and women. The rural–urban difference reached its peak in men in the years 1996–1998, when it was 6.7 (95% confidence interval [CI] 5.1–8.4) per 100,000; the corresponding figure in women was 1.6 (0.4–2.8) per 100,000. However, by 2004–2006 the rural–urban differences had almost disappeared (0.9 [−0.9 to 2.8] per 100,000 men and 0.6 [−0.7 to 1.8] per 100,000 women).

The reduction in rural–urban differences in overall suicide rates was largely attributable to the disproportionately greater rise in charcoal-burning suicide in urban than rural areas (Figure 4B), whilst the rural–urban differences in non-charcoal-burning suicide persisted throughout the study period (Figure 4C). Rates of non-charcoal-burning suicide increased during the 1990s but stabilised after 1998, when the epidemic of charcoal-burning suicide emerged. The patterns were little changed when excluding undetermined deaths or including accidents by pesticide poisoning and suffocation (unpublished data).
Discussion
The recent epidemic of suicide by charcoal burning in Taiwan showed a distinct spatiotemporal pattern in its emergence. The epidemic emerged more prominently in urban areas and there was no evidence for a single geographic area of origin. Rates of charcoal-burning suicide were consistently higher in the metropolitan and city regions than in rural areas. The reduction in rural–urban differences in overall suicide rates since around 2000 appeared to be attributable to the epidemic of charcoal-burning suicide that emerged to a greater extent in urban than rural areas.
Strengths and Limitations
This study is, to our knowledge, the first national investigation of the geographic patterning of a major epidemic of suicide. The availability of township-level data allowed a detailed investigation of the geographic distribution of the epidemic across small areas. We used Bayesian hierarchical models to estimate smoothed SMRs allowing for both global and local variability, and hence to tackle the problem that estimates of SMRs are imprecise in areas with small populations. However our study has a number of limitations. Not all suicides in Taiwan with ICD-9 codes E952/E982 are charcoal-burning suicides: a proportion will be from poisoning using other sources of nondomestic gas such as car exhaust fumes. However, data for 2002 indicate that only 10% of E952/E982 cases died from car exhaust gassing [14], although this proportion may have changed over time and thus affected the estimated contribution of charcoal-burning suicide to suicide rates by nondomestic gas poisoning. Not all undetermined deaths will be suicides [13], but the sensitivity analyses on recorded suicides alone gave similar results. The measurement of urbanisation is complex. Our indicator is the one used by the Taiwanese government and is a synthesis of previously agreed measures [15].
Possible Explanations for the Spatial Patterning of Charcoal-Burning Suicide
The epidemic of charcoal-burning suicide in Taiwan appeared to begin in mainly West Taiwan. The lack of a single area of origin is compatible with a diffuse geographic effect of media publicity and imitation [9]. Furthermore, throughout the epidemic high rates appeared to cluster in major metropolitan and city regions. This clustering indicates that the effect of media was greater in urban areas or that the method was more easily available/easier to implement in these areas. The urban environment (e.g., higher levels of media exposure and easy access to barbecue charcoals [1]) or certain characteristics of the vulnerable population living in cities (e.g., rapid acquisition of knowledge and accepting attitude towards a new suicide method [3]) may have contributed to the observed geographic distribution.
The stories of charcoal-burning suicide in television news, newspapers, and Internet articles may have triggered imitative suicides that occurred across geographic boundaries [3]. It has been suggested that the sensational coverage of charcoal-burning suicides and the detailed portrayal of the method by media may have contributed to the epidemic in Hong Kong [1],[5]. A study of suicide attempters using charcoal burning in Hong Kong showed that nearly all survivors learnt of the method from the newspaper [5]. The first charcoal-burning suicide victim in Taiwan reportedly gained knowledge of the method from a Hong Kong newspaper website [28]. Although there has been no study investigating the impact of the media's reporting style on the development of the epidemic of charcoal-burning suicide in Taiwan, a recent study shows that Taiwanese media coverage of a celebrity's suicide in 2008 was sensational and included details of the method used (charcoal burning) [29]. Such reporting is believed to contribute to the risk of imitative suicides; indeed the study also found that suicide attempters using the same method as the celebrity's suicide (charcoal burning) were more likely to report being influenced by the media coverage than those using other methods [29].
The concentration of charcoal-burning suicides in the major metropolitan and city areas of Taiwan suggests that the impact of media may be greatest in these urban regions. The finding of higher rates of charcoal-burning suicide in urban areas was not an artefact of higher underlying suicide rates, because the proportions of charcoal-burning suicide consistently showed an urban–rural gradient (Table 1). This gradient indicates that vulnerable populations in urban areas may have adopted the new suicide method more readily than their rural counterparts. Residents living in urban regions may be exposed to the television or newspaper reporting more frequently than those living in rural areas. For example, in the capital Taipei city, 92% and 66% of households were regular consumers of cable TV and newspapers, respectively, in 2000; the corresponding figures for Nantou, a rural county of central Taiwan, were 63% and 37% [30]. Urban areas also had easier access to Internet than rural areas: in 2003, a government report showed that 73% of the households were connected to Internet cable in Taipei city, compared with 25% in Nantou county [31].
In Taiwan, barbecue charcoals are mostly sold in supermarkets or convenience stores, which are mainly located in urban or suburban areas. Therefore at-risk urban residents may have easier access to the method than those living in rural areas when charcoal burning is the choice of suicide method. In Hong Kong, 80% of the charcoal-burning suicides occurred in urban areas [1]. The urban overrepresentation of charcoal-burning suicides is thought to be associated with easy access to barbecue charcoals, which are readily available in supermarkets [1]. Past research in Taiwan indicates that accessibility to lethal methods is associated with method-specific suicide rates. At county level, rates of suicide by solids/liquids poisoning (most of these suicide incidents involved pesticides) were correlated with the proportion of agricultural population, an indicator of accessibility to pesticide, and suicide rates by jumping were correlated with the proportion of households living in high buildings, an indicator of accessibility to high places to jump from [32]. Area differences in method-specific suicide rates were also seen across different countries in the world [33] and across smaller areas within one country [34] or region [35]. The differences are thought to be mainly due to different accessibility to lethal methods of suicide [33]–[35].
The Impact of Charcoal-Burning Suicide on Trends in Rural–Urban Differences
The rural excess in suicide risk prior to the appearance of charcoal-burning suicides was greatly reduced when the epidemic emerged more prominently in urban than rural areas of Taiwan. This trend was in contrast to what occurred in several western countries in recent decades. In the West, rises in suicide rates, particularly for males, were greater in rural than urban areas [36]–[39], and the rural–urban differences appeared to widen in some countries [36],[39]–[41]. In England and Wales, unfavourable trends in suicide for young people generally occurred in areas remote from main populated centres and the patterns could not be explained by changes in the lethality of popular suicide methods [38]. In contrast, our results showed that the area difference in rates of suicide by charcoal burning in Taiwan had a large impact on the rural–urban difference in overall suicide rates.
Implications for Suicide Prevention
Taiwan has experienced an upward trend in suicide rates since the early 1990s. Rises in unemployment may have contributed to these increases, although unemployment rates declined after reaching a peak around 2002 [42],[43]. The emergence of charcoal-burning suicides contributed to recent increases in suicide rates in Taiwan. In both Hong Kong and Taiwan, the emergence of charcoal-burning suicides was not accompanied by corresponding increases in suicides by other methods [3],[27]. Furthermore, charcoal-burning suicides showed different sex and age patterns from those of suicides by other methods [13],[27] and had a distinct geographic distribution, as demonstrated in our study. These observations suggest that many victims of charcoal-burning suicide would not otherwise have died by suicide if this novel method were not available. Prevention measures targeted at the method may help reverse the recent rises in suicide rates in Taiwan.
The geographic pattern of the epidemic of charcoal-burning suicide suggests that media coverage and easy assess to barbecue charcoal may have contributed to the epidemic. A better understanding of the causes of this epidemic will inform suicide prevention in Taiwan, particularly in urban areas where risk is concentrated, and has implications for other countries wishing to avoid such a public health disaster. Responsible media reporting of suicide stories, following guidelines that are now readily available [44],[45], may help prevent the spread of a new suicide method. Restricting the access to barbecue charcoals, particularly in urban areas of Taiwan, with measures such as placing charcoal bags behind supermarket counters or banning the sale in convenience stores may also help offset the unfavourable trends [1],[5]. Responsible media reporting is essential to prevent the spread of a new suicide method with high lethality such as charcoal burning in regions where this suicide method is not yet widely known [1]. However, in countries like Taiwan where the epidemic of charcoal-burning suicide is already established, the controls of environmental factors such as access to barbecue charcoal may be more effective since it takes time for the perception of this particular method of suicide to be changed by responsible media reporting and public education [1]. The distinct spatiotemporal pattern of charcoal-burning suicide in Taiwan shown here has potential public health implications for comprehensive suicide prevention strategies.
Supporting Information
Zdroje
1. YipPS
LeeDTS
2007 Charcoal-burning suicides and strategies for prevention. Crisis 28 Suppl 1 21 27
2. LeeDT
ChanKP
LeeS
YipPS
2002 Burning charcoal: a novel and contagious method of suicide in Asia. Arch Gen Psychiatry 59 293 294
3. LiuKY
BeautraisA
CaineE
ChanK
ChaoA
2007 Charcoal burning suicides in Hong Kong and urban Taiwan: an illustration of the impact of a novel suicide method on overall regional rates. J Epidemiol Community Health 61 248 253
4. LinJJ
LuTH
2008 Suicide mortality trends by sex, age and method in Taiwan, 1971–2005. BMC Public Health 8 6
5. ChanKP
YipPS
AuJ
LeeDT
2005 Charcoal-burning suicide in post-transition Hong Kong. Br J Psychiatry 186 67 73
6. HuhGY
JoGR
KimKH
AhnYW
LeeSY
2009 Imitative suicide by burning charcoal in the southeastern region of Korea: the influence of mass media reporting. Leg Med (Tokyo) 11 S563 S564
7. PatelF
2008 Carbon copy deaths: carbon monoxide gas chamber. J Forensic Leg Med 15 398 401
8. LinJJ
LuTH
2008 High-risk groups for charcoal-burning suicide in Taiwan, 2001-2005. J Clin Psychiatry 69 1499 1501
9. JoinerTE
1999 The clustering and contagion of suicide. Curr Dir Psychol Sci 8 89 92
10. CantorCH
BaumePJ
1998 Access to methods of suicide: what impact? Aust N Z J Psychiatry 32 8 14
11. LinsleyKR
SchapiraK
KellyTP
2001 Open verdict v. suicide - importance to research. Br J Psychiatry 178 465 468
12. OhbergA
LonnqvistJ
1998 Suicides hidden among undetermined deaths. Acta Psychiatr Scand 98 214 218
13. ChangSS
SterneJA
LuTH
GunnellD
2009 ‘Hidden’ suicides amongst deaths certified as undetermined intent, accident by pesticide poisoning and accident by suffocation in Taiwan. Soc Psychiatry Psychiatr Epidemiol. In press
14. LinJJ
ChenLH
HuangSM
LuTH
2008 Problems in estimating the number of suicides by charcoal burning in Taiwan. J Epidemiol Community Health 62 566
15. LiuCY
HungYT
ChuangYL
ChenYJ
WengWS
2006 Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J Health Management (Chin) 4 1 22
16. Construction and Planning Agency, Taiwan 2001 Urban planning. Available: http://www.cpami.gov.tw/web/index.php?option=com_content&task=view&id=1126&Itemid=75. Accessed 1 May 2009
17. AssuncaoRM
ReisEA
1999 A new proposal to adjust Moran's I for population density. Stat Med 18 2147 2162
18. AnselinL
SyabriI
KhoY
2006 GeoDa: An introduction to spatial data analysis. Geogr Anal 38 5 22
19. ClaytonD
KaldorJ
1987 Empirical Bayes estimates of age-standardized relative risks for use in disease mapping. Biometrics 43 671 681
20. LawsonAB
BiggeriAB
BoehningD
LesaffreE
VielJF
2000 Disease mapping models: an empirical evaluation. Disease Mapping Collaborative Group. Stat Med 19 2217 2241
21. MiddletonN
SterneJA
GunnellDJ
2008 An atlas of suicide mortality: England and Wales, 1988–1994. Health Place 14 492 506
22. MollieA
2000 Bayesian mapping of Hodgkin's disease in France.
ElliotP
WakefieldJC
BestNG
BriggsDJ
Spatial epidemiology: methods and applications Oxford Oxford University Press 267 285
23. GilksWR
RichardsonS
SpiegelhalterDJ
1996 Markov chain Monte Carlo in practice. London Chapman & Hall
24. ThomasA
BestN
LunnD
ArnoldR
SpiegelhalterD
2003 GeoBUGS user manual, version 1.2. Cambridge MRC Biostatistics Unit
25. BrooksSP
GelmanA
1998 General methods for monitoring convergence of iterative simulations. J Comput Graph Stat 7 434 455
26. BrewerCA
MacEachrenAM
PickleLW
HerrmannD
1997 Mapping mortality: evaluating color schemes for choropleth maps. Ann Assoc Am Geogr 87 411 438
27. PanY-J
LiaoS-C
LeeM-B
2009 Suicide by charcoal burning in Taiwan, 1995–2006. J Affect Disord. In press
28. Mingpaonews 2000 Under the influence of internet information from Hong Kong, the first case of charcoal burning suicide emerged in Taiwan. Mingpaonews.
29. ChenYY
TsaiPC
ChenPH
FanCC
HungGC
2009 Effect of media reporting of the suicide of a singer in Taiwan: the case of Ivy Li. Soc Psychiatry Psychiatr Epidemiol In press
30. Directorate-General of Budget Accounting and Statistics, Taiwan 2000 National statistics. Important indicators for each county. Available: http://61.60.106.82/pxweb/Dialog/statfile9.asp. Accessed 5 May 2009
31. Research Developmennt and Evaluation Commission, Taiwan 2002 Digital divide in Taiwan, 2002. Available: http://www.rdec.gov.tw/ct.asp?xItem=4024389&ctNode=11171. Accessed 5 May 2009
32. LinJJ
LuTH
2006 Association between the accessibility to lethal methods and method-specific suicide rates: an ecological study in Taiwan. J Clin Psychiatry 67 1074 1079
33. Ajdacic-GrossV
WeissMG
RingM
HeppU
BoppM
2008 Methods of suicide: international suicide patterns derived from the WHO mortality database. Bull World Health Organ 86 726 732
34. LevinKA
LeylandAH
2005 Urban/rural inequalities in suicide in Scotland, 1981–1999. Soc Sci Med 60 2877 2890
35. MarzukPM
LeonAC
TardiffK
MorganEB
StajicM
1992 The effect of access to lethal methods of injury on suicide rates. Arch Gen Psychiatry 49 451 458
36. MehlumL
HyttenK
GjertsenF
1999 Epidemiological trends of youth suicide in Norway. Arch Suicide Res 5 193 205
37. PesonenTM
HintikkaJ
KarkolaKO
SaarinenPI
AntikainenM
2001 Male suicide mortality in eastern Finland–urban-rural changes during a 10-year period between 1988 and 1997. Scand J Public Health 29 189 193
38. MiddletonN
GunnellD
FrankelS
WhitleyE
DorlingD
2003 Urban-rural differences in suicide trends in young adults: England and Wales, 1981-1998. Soc Sci Med 57 1183 1194
39. RazvodovskyY
StickleyA
2009 Suicide in urban and rural regions of Belarus, 1990-2005. Public Health 123 27 31
40. SinghGK
SiahpushM
2002 Increasing rural-urban gradients in US suicide mortality, 1970-1997. Am J Public Health 92 1161 1167
41. KapustaND
ZormanA
EtzersdorferE
Ponocny-SeligerE
Jandl-JagerE
2008 Rural-urban differences in Austrian suicides. Soc Psychiatry Psychiatr Epidemiol 43 311 318
42. ChangSS
SterneJAC
HuangWC
ChuangHL
GunnellD
2009 The association of secular trends in unemployment with suicide in Taiwan, 1959–2007: a time-series analysis. Public Health. In press
43. ChangSS
GunnellD
SterneJAC
LuTH
ChengATA
2009 Was the economic crisis 1997-1998 responsible for rising suicide rates in East/Southeast Asia? A time-trend analysis for Japan, Hong Kong, South Korea, Taiwan, Singapore and Thailand. Soc Sci Med 68 1322 1331
44. PirkisJ
BloodRW
BeautraisA
BurgessP
SkehansJ
2006 Media guidelines on the reporting of suicide. Crisis 27 82 87
45. World Health Organization 2008 Preventing suicide. A resource for media professionals. Geneva World Health Organization
Štítky
Interní lékařstvíČlánek vyšel v časopise
PLOS Medicine
2010 Číslo 1
- Alternativní léčebné možnosti u hypercholesterolemie při intoleranci statinů
- Vliv kombinace nutraceutik na remodelaci levé komory srdeční u osob s metabolickým syndromem
- Nutraceutika a jejich ovlivnění mírného kardiometabolického rizika
- Princip účinku medu v léčbě chronických i infikovaných ran
- Superoxidovaný roztok a jeho využití v léčbě ran
Nejčtenější v tomto čísle
- The Evolution of the Epidemic of Charcoal-Burning Suicide in Taiwan: A Spatial and Temporal Analysis
- Male Circumcision at Different Ages in Rwanda: A Cost-Effectiveness Study
- Geographic Distribution of Causing Invasive Infections in Europe: A Molecular-Epidemiological Analysis
- “Working the System”—British American Tobacco's Influence on the European Union Treaty and Its Implications for Policy: An Analysis of Internal Tobacco Industry Documents